PHOENIX — On a normal July 4th weekend, the main difference between a backyard barbecue and a West Nile virus exposure is whether the hosts remembered to empty the birdbath. This year, the Centers for Disease Control and Prevention would like everyone to remember the birdbath.
Data released by the CDC shows that as of June 30, 48 people in the United States had been confirmed with West Nile virus, 38 of them with neuroinvasive disease, the form of the infection that crosses into the central nervous system and can cause encephalitis, meningitis, or permanent paralysis. The historical average for confirmed cases by the close of June is roughly 10, measured since modern tracking began in 2004. The agency says this is the worst early start to West Nile season in more than two decades.
The geographic core of the outbreak is Maricopa County, Arizona. Of 48 national cases, 29 are in a single county, the Phoenix metropolitan area, where 4 people have already died. Arizona’s climate, laced with irrigated landscapes and agricultural canals that create standing water for Culex quinquefasciatus mosquitoes year-round, has made Maricopa County one of the country’s most consistent West Nile hotspots since the virus first arrived in the United States in 1999. What is different about 2026 is how early and how severely it has begun.
Dr. Erin Staples, a CDC expert in insect-borne diseases, said last week that “these findings serve as an important reminder that mosquito season is well underway.” That statement arrived 23 states deep and before the July 4th holiday, when millions of Americans will spend evening hours outside during the hours Culex mosquitoes feed most actively. The numbers behind it: 23 states reporting West Nile virus cases before the end of June is the widest geographic spread for that point in the year in a decade.
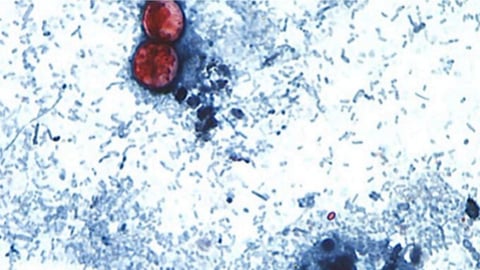
The transmission mechanism is straightforward enough that the problem is structural, not mysterious. West Nile virus lives primarily in bird populations, where most infected birds carry it without becoming sick. A Culex mosquito feeds on an infected bird and picks up the virus; that same mosquito feeds on a human and passes it. Most people who are infected never know it; the CDC estimates that only about 20 percent develop any symptoms at all. Roughly one in 150 infections progresses to neuroinvasive disease. But when the season opens with 38 neuroinvasive cases before July, that ratio produces a visible toll quickly.
The same avian populations that serve as West Nile’s reservoir hosts are also part of the ecological networks now carrying high-pathogenicity avian influenza to previously unaffected regions. Australia confirmed its first HPAI designation in late June, triggering poultry lockdowns across Western Australia. The dynamics are entirely different: bird flu infects and sickens birds, while West Nile circulates through them silently. Both diseases are reminders that wild bird populations form part of the infrastructure through which pathogens move between species.

The CDC’s prevention advice has been consistent for years, and its consistency is also part of the challenge in communicating it urgently. Use an EPA-registered insect repellent containing DEET, picaridin, or oil of lemon eucalyptus. Wear long sleeves and pants outdoors during evening hours. Remove standing water from any container in the yard. Fix broken window screens. Avoid outdoor activities at dusk and dawn. Melissa Kretschmer, a public health official in Maricopa County, offered a detail that collapses the scale of the problem into a manageable physical object: “Even an overturned bottle cap can hold enough water for mosquitoes to breed.” According to the CDC’s prevention guidance, no vaccine or preventive medicine exists for humans; protection depends entirely on reducing the chance of being bitten.
West Nile season runs from June through October, with the largest case concentrations historically arriving in August and September. The 2026 season began at a pace not seen this early since 2004, the worst outbreak in American history, which produced more than 2,500 neuroinvasive cases and more than 100 deaths by year’s end. Whether 2026 will reach anywhere near that scale is not something June 30 data can answer. What it can say is that the trajectory heading into peak season is steeper than anything recorded in the past two decades.
The CDC’s ArboNET surveillance system tracks reported West Nile cases in real time through late fall. The 48 confirmed cases represent only a fraction of actual infections; the CDC estimates that reported cases account for roughly one in 30 total infections, meaning the true infection count in the United States as of June 30 is likely in the thousands, the vast majority of whom experienced no symptoms or a brief flu-like illness and were never tested.
The category that public health officials are watching most closely is neuroinvasive disease. West Nile can cause encephalitis, meningitis, or acute flaccid paralysis, a syndrome that can leave patients with permanent limb weakness. Older adults and people with weakened immune systems face higher risks of developing the severe form; transplant recipients on immunosuppressive medications are among those for whom a mosquito bite carries an elevated risk of serious illness. There is no antiviral treatment. Clinical management is supportive.
What the data cannot yet explain is why this season began so early and so severely. Temperature and rainfall patterns influence mosquito populations significantly, and environmental conditions that generate large pools of standing water can produce rapid breeding surges. Whether the 2026 early surge reflects those conditions, changes in surveillance sensitivity, or some combination is part of what epidemiologists are working to understand. The 4th of July weekend is not waiting for that answer.