
A major shift in endocrine medicine is reshaping how one of the most widely diagnosed conditions in women is understood, treated, and discussed. Polycystic Ovary Syndrome, long abbreviated as PCOS, has officially been renamed Polyendocrine Metabolic Ovarian Syndrome, or PMOS, in a move driven by mounting evidence that the old terminology failed to capture the full biological complexity of the disorder.
The renaming follows years of debate within the global medical community, culminating in what researchers describe as an international consensus involving leading endocrine experts. The central argument is straightforward. The previous label overstated ovarian appearance while underrepresenting systemic hormonal and metabolic dysfunction.
Under the new framework, PMOS is defined as a multisystem condition affecting endocrine regulation, metabolic stability, and reproductive function. This reframing is not semantic. It directly alters how clinicians evaluate long-term risk and design treatment strategies.
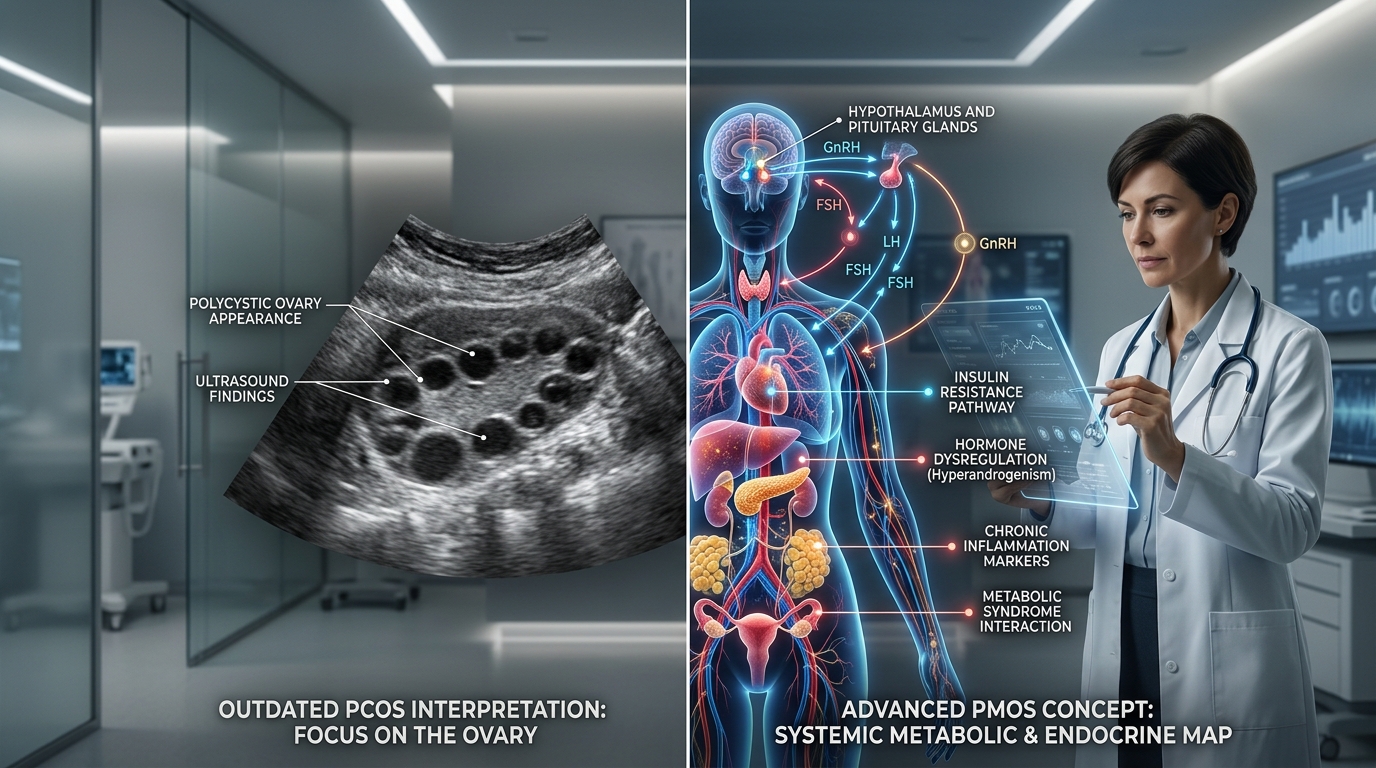
For decades, patients were told they had a gynecological condition defined by ovarian “cysts.” In practice, many of these structures are immature follicles rather than true cysts, and some patients show no such features at all. Critics argue that this has contributed to widespread diagnostic confusion and delayed treatment, reinforcing a distorted public understanding of the disorder.
Medical researchers now emphasize that PMOS is better understood as a systemic condition affecting multiple organs and regulatory pathways. This includes a broad range of metabolic disruptions, particularly involving insulin signaling, lipid regulation, and long-term cardiovascular risk.

One of the most significant clinical concerns is insulin resistance, which is now recognized as a central driver of disease progression in many patients. The condition is frequently associated with weight gain, glucose dysregulation, and elevated risk of Type 2 diabetes. Modern treatment approaches increasingly incorporate metabolic intervention strategies targeting insulin resistance and metabolic risk in PMOS.
Globally, the scale of the condition is substantial. Epidemiological estimates suggest it affects approximately 170 million people worldwide, making it one of the most common endocrine disorders affecting women of reproductive age.
Despite its prevalence, diagnosis has historically been inconsistent. Clinical guidelines continue to rely on established criteria that evaluate irregular ovulation, androgen excess, and ovarian morphology. These standards are outlined in current diagnostic criteria for PCOS and PMOS, though experts acknowledge they are evolving alongside the new nomenclature.
Symptoms vary widely. Patients may experience irregular menstrual cycles, acne, excess facial hair, hair thinning, fatigue, mood disorders, and difficulties with weight regulation. The variability of presentation has long complicated diagnosis, leading many patients to undergo years of fragmented care.
The condition also carries significant reproductive implications. Ovulatory dysfunction remains one of the most common causes of infertility linked to endocrine disorders, with global health authorities noting its impact on fertility across populations.
Beyond reproduction, attention is shifting toward long-term systemic risks. Cardiovascular disease, metabolic syndrome, and psychological comorbidities are increasingly central to clinical evaluation. This broader approach is reflected in emerging guidance that emphasizes early metabolic screening rather than symptom management alone.

Therapeutic strategies are also evolving. Alongside traditional hormonal treatments, clinicians are increasingly exploring metabolic interventions, including drugs originally developed for diabetes and obesity management. Interest in GLP-1 medications has grown as evidence suggests potential benefits in addressing insulin resistance and weight-related complications.
Experts describe the renaming as part of a broader correction in how medicine conceptualizes women’s health conditions. For decades, critics argue, complex endocrine disorders were oversimplified into reproductive categories, limiting both research funding and clinical innovation.
The implications of PMOS extend beyond terminology. They reflect a shift toward recognizing interconnected biological systems rather than isolated organ dysfunction. In this framework, ovarian symptoms are understood as one expression of a broader metabolic and endocrine imbalance.

What remains unresolved is how quickly clinical practice will adapt. For millions of patients worldwide, the change offers validation, but also raises new expectations for earlier diagnosis, more integrated treatment, and a medical system that finally reflects the complexity of their condition.