
GLASGOW — For decades, engineers designing implantable medical devices have run into the same wall: wireless communication requires antennas, and the antennas that work inside the body are too large, too hot, or too power-hungry to be practical in the places they are needed most. A research team at the University of Glasgow may have a way through it.
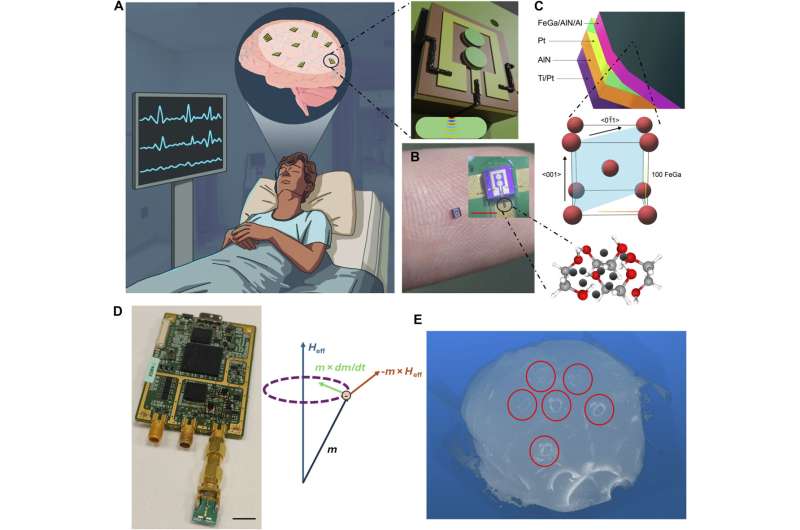
The team’s new design, published Thursday in Science Advances, describes a type of antenna called µBots (microbots) that measures less than a millimeter across but achieves bandwidths up to 22.6 gigahertz, enough to transmit sonogram video and audio signals in real time through living tissue. The underlying trick is borrowed from acoustics: rather than relying purely on electromagnetic radio frequency methods, the antennas exploit acoustic resonances in the device substrate to generate signal overtones that carry both power and data. That makes them substantially smaller, lighter, and cooler than conventional radio-frequency antennas of equivalent capability.
Heat is the thing that conventional implantable wireless hardware cannot escape. RF antennas efficient enough to reach the bandwidth requirements of real-time biomedical monitoring generate enough thermal energy to damage surrounding tissue, which sets a hard ceiling on what can be put inside the brain long-term. The µBot architecture sidesteps that limit by switching physics: acoustic overtones in the substrate carry the signal load, letting the electromagnetic component operate at a lower intensity and generate less waste heat in the surrounding biological environment.
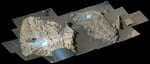
In testing, a single µBot met the bandwidth benchmarks the team was targeting, and an array of nine devices in a phased configuration matched the alignment performance of a single conventional large RF antenna while fitting inside a far smaller footprint. The researchers validated results in rat brain tissue, human cortical brain slices, and controlled cell cultures, three layers of biological testing that suggest the antenna behavior holds up in environments that approximate the electrical properties of the human brain.
The applications the team has in mind are specific and serious. Neurological conditions where continuous real-time monitoring or on-demand intervention is valuable include epilepsy, where a device could detect and respond to seizure precursors before they develop; Parkinson’s disease, where neuromodulation currently requires bulky external hardware; and neurodegenerative diseases, where early biochemical markers in the brain are difficult to track without invasive measurement apparatus. The µBots, if they clear development, would let a device sit fully inside the body and communicate wirelessly without the tether or recharging constraints that currently limit what is clinically possible.
Dr. Mahdieh Shojaei Baghini, the corresponding author and a researcher at the James Watt School of Engineering, said the team treats the device substrate as an active contributor to signal generation rather than passive mounting infrastructure. “The µBots we’re developing harness the potential of acoustic resonance to address many of the issues which have held back the technology to date,” she said, pointing to heat generation and antenna size as the two constraints the design specifically targets.
The research emerged from an international collaboration that included the University of Modena and Reggio Emilia, Harvard Medical School, and five additional European research centers. Funding came from the European Innovation Council’s Pathfinder Challenge program through the CROSSBRAIN project and separately from the Advanced Research and Invention Agency’s NEUROBOT initiative and the U.S. National Science Foundation. The breadth of the funding sources reflects a convergence of European and American interest in solving the implantable device bottleneck for neurological applications specifically.
The neurological disease context matters for understanding the clinical stakes. Treatments for conditions like Parkinson’s and Huntington’s disease are increasingly moving toward precision approaches, genetic therapies and targeted neuromodulation, but their delivery and monitoring systems have not kept pace with what the underlying science now demands. Earlier this year, a gene therapy trial for Huntington’s disease showed a 75 percent slowdown in disease progression, a landmark result that depends on hardware capable of real-time monitoring to deploy safely and effectively at scale. The µBot architecture is designed for exactly that kind of supporting role.
The gap between laboratory performance and a clinical implant is, however, considerable. The µBots have been tested in tissue, not in living patients, and the path from tissue validation to a human implant involves biocompatibility testing over months and years, regulatory submissions that take longer still, and the engineering challenge of integrating the antenna with a power source, signal processor, and drug-delivery or neuromodulation actuator in something that fits inside a surgical implant. The paper does not address any of those downstream steps. What it provides is a demonstrated antenna architecture that removes one of the principal obstacles to getting there.
Neuromodulation for Parkinson’s disease offers a concrete reference point for what success would look like. Deep brain stimulation, the current standard approach, requires a device implanted in the skull connected by wires to a battery pack under the collarbone, a system that works but imposes physical constraints and failure modes that a fully wireless alternative would avoid. Research from 2023 explored new approaches to Parkinson’s neuromodulation that pointed toward wireless as a necessary direction, without the hardware to achieve it at the implant scale. The µBot design addresses the core antenna problem that has made that direction difficult to build.
What remains open is whether the acoustic resonance approach scales. Whether the same architecture that works at 22.6 gigahertz in a lab can be manufactured reliably at the tolerances required, in quantities that make clinical devices commercially viable, is a question the publication does not reach. The µBot is a design, demonstrated in tissue, that solves the wireless implant antenna problem in one configuration. Whether it solves it well enough to survive contact with the engineering and regulatory system that turns laboratory results into clinical medicine is what the team has yet to be asked to answer.