
The long-promised breakthrough in Alzheimer’s treatment is now facing a stark and uncomfortable reckoning.
A sweeping new analysis of more than 20,000 patients has concluded that drugs designed to remove amyloid plaques from the brain — once heralded as the most promising path to slowing dementia — deliver effects so small they are, in clinical terms, barely perceptible. The finding is not merely incremental. It cuts to the core of a scientific doctrine that has dominated Alzheimer’s research for decades.
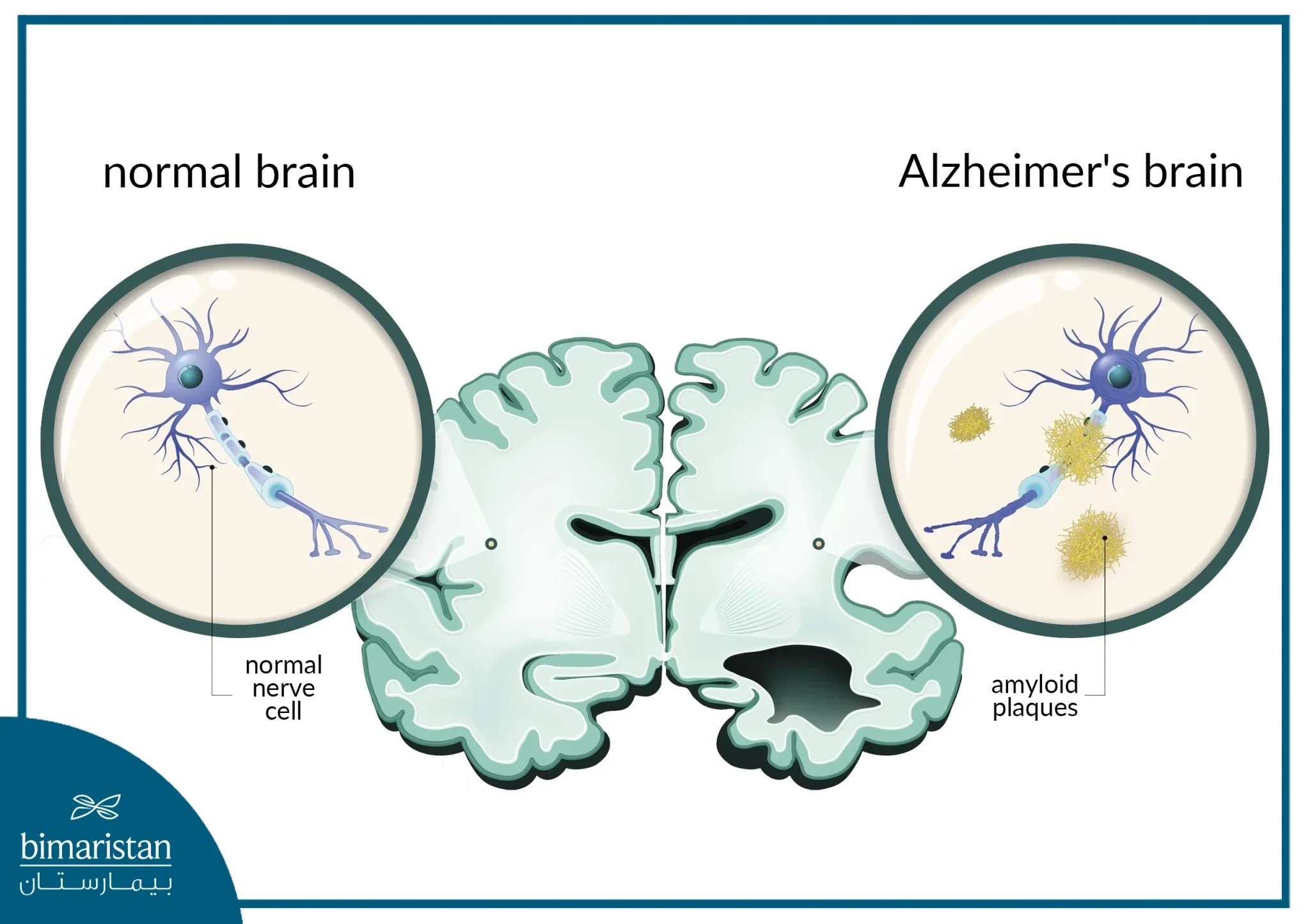
At the center of the controversy is a Cochrane review, widely regarded as the gold standard in evidence synthesis, which examined 17 clinical trials spanning roughly 18 months. Its conclusion was blunt: anti-amyloid therapies showed “no clinically meaningful effect” on cognitive decline or dementia severity, despite successfully clearing amyloid buildup in the brain.
This is the paradox now confronting the field. The drugs appear to do exactly what they were designed to do — remove amyloid plaques — yet patients do not meaningfully improve.

Now, that premise is under renewed scrutiny.
“Successful removal of amyloid does not seem to be associated with clinically meaningful effects,” researchers concluded, underscoring a widening gap between biological success and patient outcomes.
The implications are profound. If amyloid removal does not translate into tangible cognitive benefits, the entire therapeutic strategy may require rethinking.
Yet the science is far from settled — and the backlash has been swift.
Critics argue that the review paints an overly pessimistic picture by aggregating data from both outdated, ineffective drugs and newer therapies such as lecanemab and donanemab, which have shown modest but statistically significant benefits in recent trials. Only a small fraction of the analyzed studies included these next-generation treatments, potentially diluting their apparent impact.
Those newer drugs, while far from curative, have been approved in several markets and were initially hailed as the first disease-modifying therapies for Alzheimer’s. In controlled trials, drugs slowed cognitive decline by only a fraction in clinical trials — a modest gain, but one that some clinicians argue is meaningful for patients and families navigating a relentless disease.
Even so, regulators have hesitated. In the UK, health authorities declined to fund these treatments through public systems, citing limited benefit relative to their high cost and the logistical burden of administration, which often requires frequent infusions and ongoing brain scans.

The broader scientific unease extends beyond clinical trial results. Recent reporting has highlighted deeper cracks in the amyloid hypothesis itself, including controversies over foundational research and the retraction of influential studies that once reinforced the theory’s dominance.
Taken together, these developments are fueling a growing sense that Alzheimer’s may be far more complex than a single protein-driven disease.
Some researchers now argue that amyloid is only one piece of a larger pathological puzzle — perhaps a byproduct rather than the root cause. Others suggest that timing is critical: removing amyloid after symptoms appear may simply be too late, akin to intervening after irreversible neuronal damage has already occurred. Emerging evidence suggests that early treatment to remove amyloid plaques may delay onset, pointing to a narrower therapeutic window.
There is also a strategic pivot underway. Scientists are increasingly exploring alternative targets, including tau proteins, neuroinflammation, and the brain’s immune system. This development reshapes the broader landscape of Alzheimer’s research and dementia treatment breakthroughs.
At the same time, parallels are emerging across modern medicine. The limitations of modern medicine and breakthrough narratives are becoming harder to ignore, as high-profile drugs fail to deliver uniform outcomes across populations.
And the uncertainty is not confined to neurology. Broader growing concerns about medical reliability and emerging technologies are raising fundamental questions about how innovation is evaluated and deployed in healthcare systems worldwide.
Still, even proponents of the amyloid approach concede that it is unlikely to be a complete solution.
“Anti-amyloid treatments will not be the whole answer,” experts have acknowledged, emphasizing the need for a broader, multi-targeted strategy.
For patients and families, the stakes could not be higher. Alzheimer’s remains one of the most devastating neurodegenerative diseases, affecting more than 55 million people worldwide. The urgency to find effective treatments is matched only by the complexity of the disease itself.
What emerges from this latest evidence is not a definitive verdict, but a turning point. The field is entering a phase of introspection — one that may ultimately prove as consequential as any breakthrough.
The question is no longer just whether amyloid can be removed.
It is whether removing it was ever enough.