BUNIA, Democratic Republic of the Congo — The treatment center in Ituri province that enrolled its first patient on Thursday is the only site in the world currently testing experimental drugs against the Bundibugyo strain of Ebola. Six weeks into an outbreak that has infected more than 1,400 people and killed 438, clinicians across three affected provinces in eastern Congo have had only fluids, fever management, and isolation to offer. The trial does not provide an approved cure. What it does, for the first time, is create a mechanism to find one.
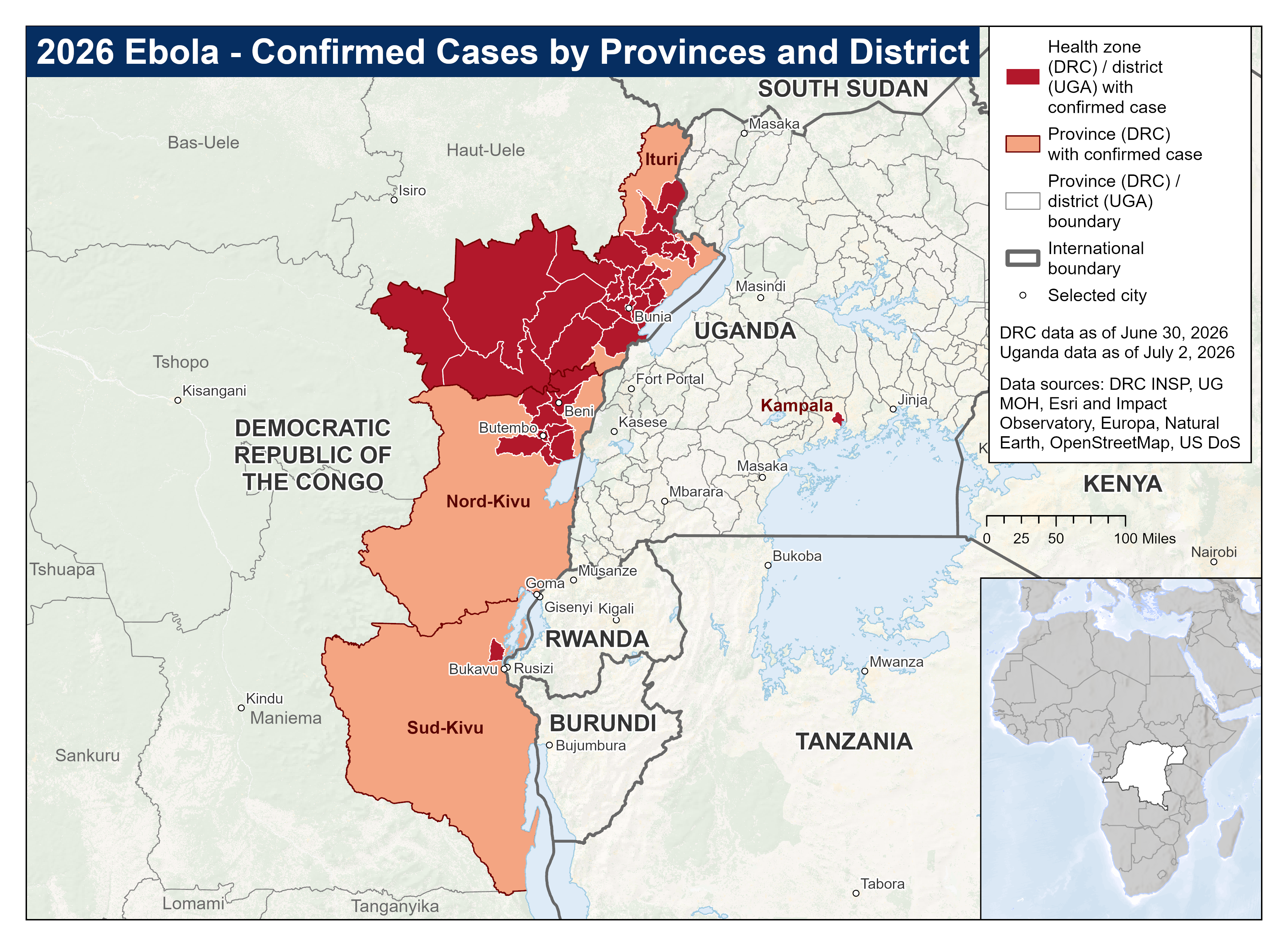
International health officials had been pressing for this research since the Bundibugyo virus disease outbreak was declared simultaneously in the Democratic Republic of the Congo and in Uganda on May 15. The World Health Organization designated it a public health emergency of international concern two days later; Africa CDC followed with a continental security declaration within 24 hours. By late June, Congo’s health ministry had confirmed more than 1,000 cases in DRC alone, with the Ituri province city of Bunia at the center and additional clusters recorded in Nord-Kivu, Sud-Kivu, and Uganda’s capital Kampala. The current toll makes this the third-largest Ebola outbreak ever recorded.
The trial is testing two existing drugs against the virus: remdesivir, the broad-spectrum antiviral that Gilead Sciences developed originally for COVID-19, and MBP134, an engineered antibody cocktail designed by Mapp Biopharmaceutical to target multiple Ebola strains. Researchers are also evaluating obeldesivir, a related compound, as a post-exposure prophylaxis for people exposed to the virus before symptoms appear. Each enrolled patient is randomly assigned to receive standard supportive care plus remdesivir, MBP134, both drugs, or neither. The primary measure is survival at 28 days, ABC News reported.
The trial is coordinated by the WHO, Congo’s national biomedical research institute, Oxford University, and the Antwerp-based Institute of Tropical Medicine. Researchers estimate it could require up to 1,000 participants and take several months to complete. It is currently operating from a single center in Ituri and is expected to expand to additional sites as the security situation allows.
WHO Director-General Tedros Adhanom Ghebreyesus described the launch as offering “real hope that we can deliver concrete results for, and with, the communities at the heart” of the outbreak. Africa CDC Director-General Jean Kaseya pressed harder. “We have the science. We now need the funding to use it,” he said last week. “Every day of delay costs lives we could save.”
The urgency in Kaseya’s statement was not rhetorical. Africa CDC has appealed for US$18 million to close a critical shortfall in its therapeutics program, according to an appeal published June 29. Of the $26 million total required for the full trial portfolio, only $10 million has been secured. The gap leaves $16 million in post-exposure prophylaxis studies unfunded, along with $2 to $3 million for contact tracing across the outbreak zone.
Bundibugyo is among the least-studied Ebola strains. It was first identified in Uganda in 2007 and caused a contained outbreak there between 2007 and 2008. Unlike the Zaire strain that drove the 2014 to 2016 West Africa epidemic and the 2018 to 2020 DRC outbreak that killed more than 2,200 people, Bundibugyo has received little investment in medical countermeasures. The two drugs approved for Zaire Ebola, Ebanga and Inmazeb, are not licensed for Bundibugyo, and whether they would be effective against this strain remains an open question that the current trial will not directly answer.
Thirteen African Union member states considered at elevated risk met in Kampala last week under Africa CDC’s coordination, testing contingency plans at border crossings. The group included Angola, Burundi, the Central African Republic, Ethiopia, Kenya, Rwanda, Somalia, South Sudan, Tanzania, and Zambia, countries that share land borders with DRC or Uganda or that handle significant transit from affected regions.
The scientific problem of developing effective antivirals against understudied viral strains runs well beyond Ebola. Research published this week into antiviral immune suppression mechanisms in sea anemones found that organisms can use counterintuitive strategies, including suppressing rather than activating their own immune response, to resist viral infection. Against a pathogen like Bundibugyo, where the mechanisms of immune evasion are not fully mapped and no approved treatments exist, the researchers in Ituri are collecting evidence that does not exist anywhere else.
What remdesivir and MBP134 will actually do against Bundibugyo is the question Thursday’s enrollment was designed to answer, but cannot answer yet. The trial requires the outbreak to continue long enough to accumulate participants, which is not in any patient’s interest, and it requires the $18 million funding gap to close, which has not happened. For the single center in Ituri where the 28-day survival clock is now running, both uncertainties remain.