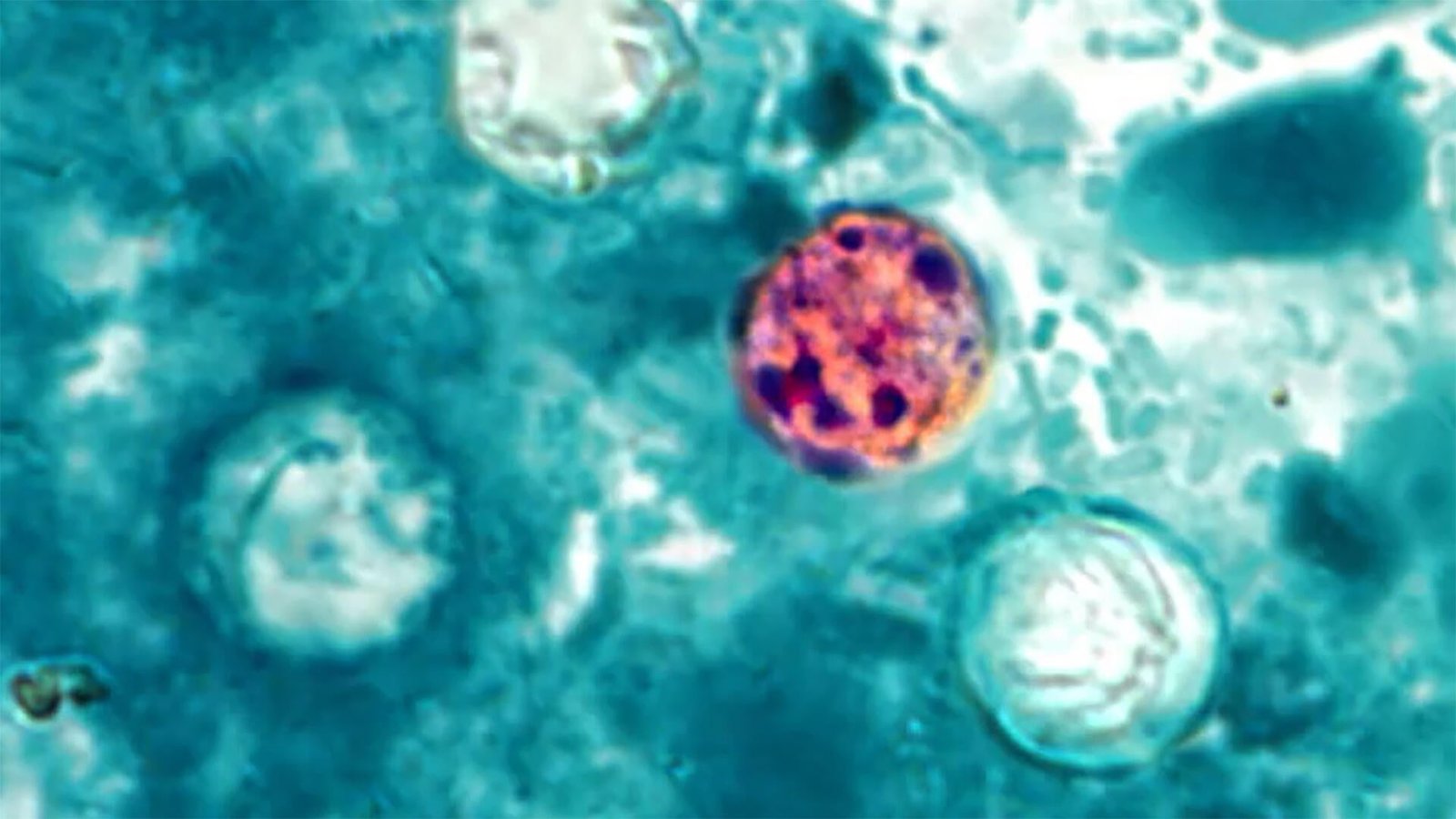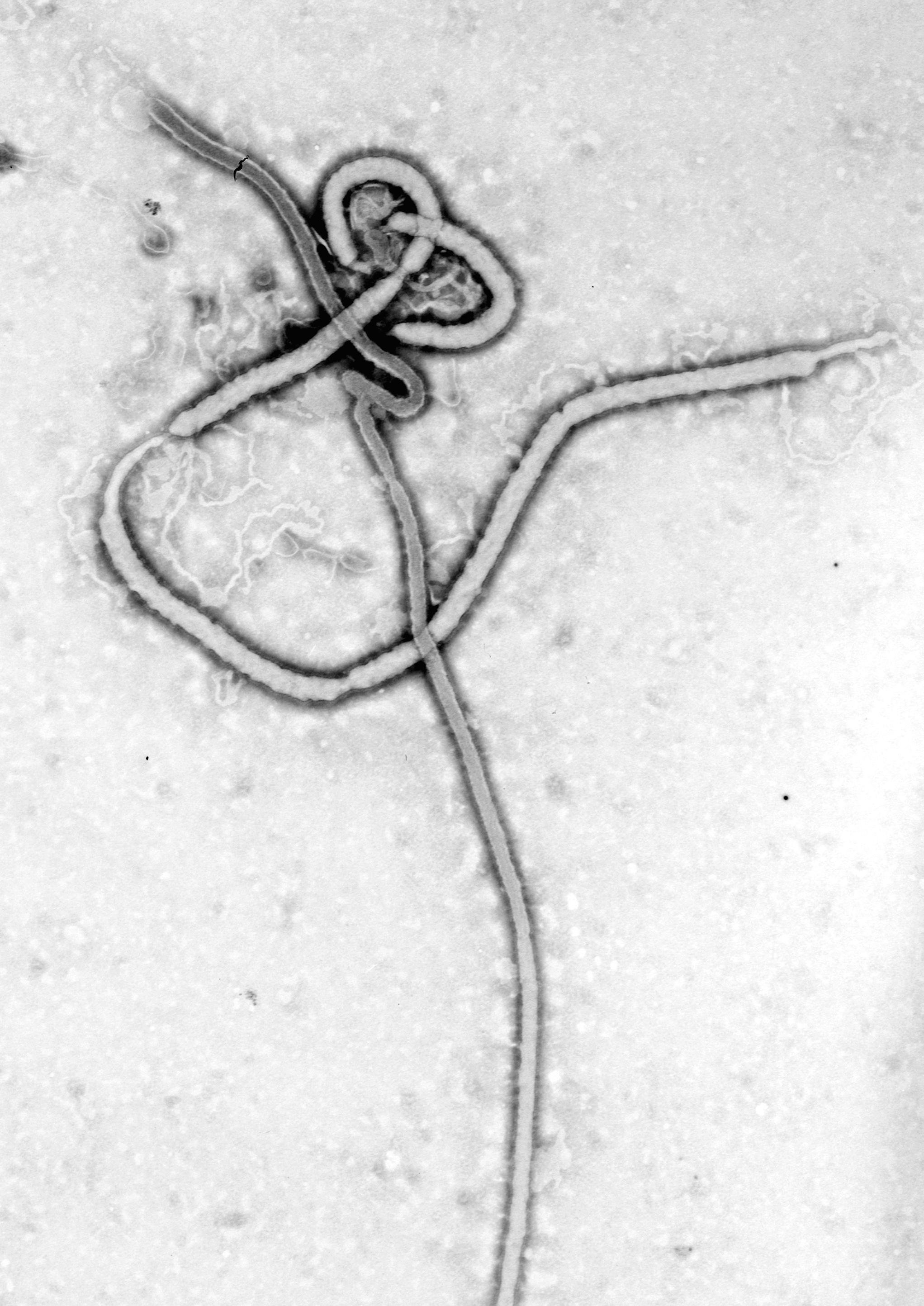

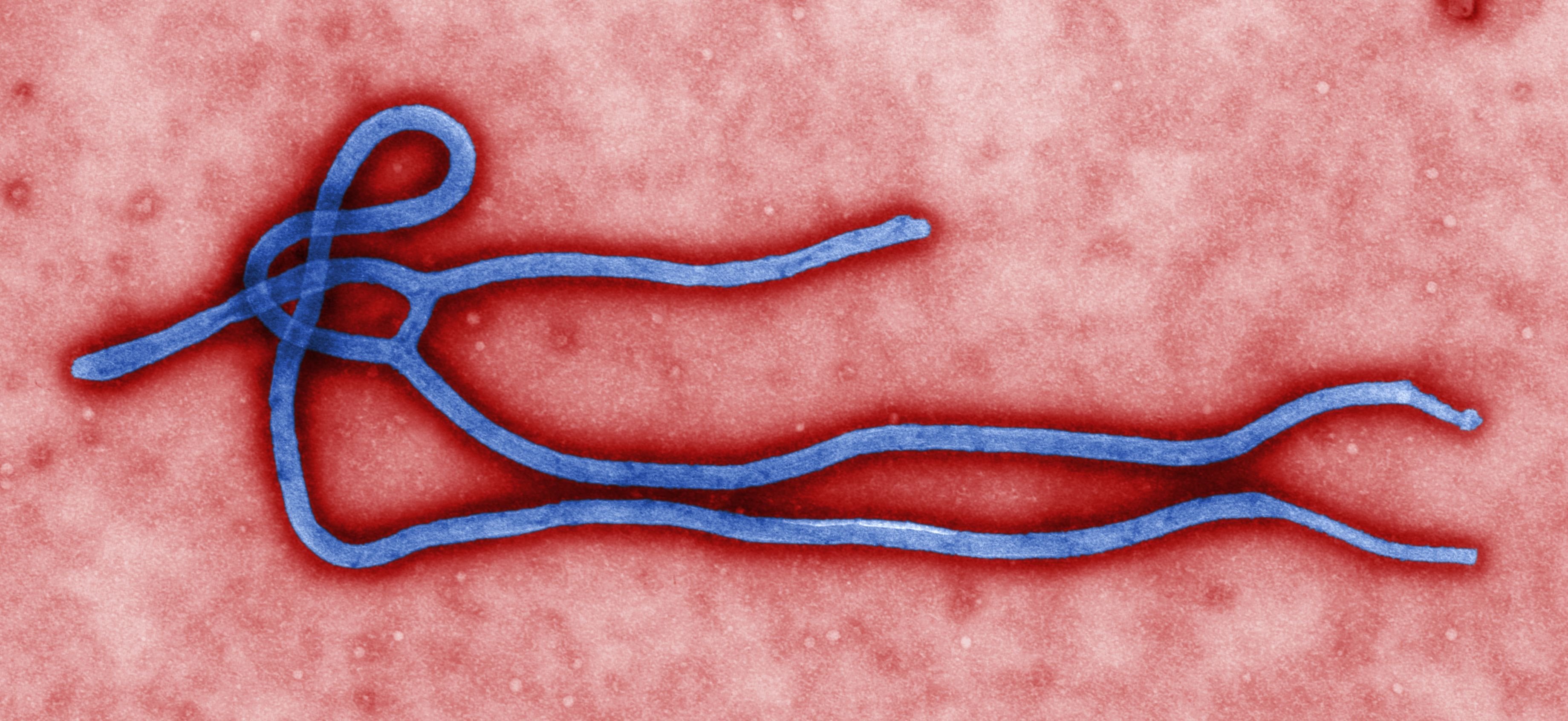
PARIS — He crossed two continents and landed at Charles de Gaulle with what felt like a headache. By the time French health authorities confirmed he was carrying the Bundibugyo strain of Ebola virus, he had spent hours on a commercial flight from Kinshasa with more than a hundred other passengers, most of whom had no reason to believe they had been near one of the deadliest pathogens known to medicine. He was a doctor. He had been on a humanitarian mission in the Democratic Republic of Congo. He came home feeling unwell.
France confirmed the case on June 24, the first Ebola infection to reach European soil in the current outbreak, which has already recorded 1,118 confirmed cases and 291 deaths in the DRC as of June 25, making it the worst Ebola outbreak in history by case numbers in its first month. Five other passengers who sat near the doctor on the flight have been identified as possible contacts and placed in 21-day isolation while health authorities determine whether the virus spread during transit. The 21-day window will not close until mid-July.
The doctor is in stable condition with a very low viral load, according to France’s health ministry, which has not released his name or the humanitarian organization he served. He is isolated at a specialized infectious-disease facility in Paris. The detail that has made public health officials watch this case carefully is not the severity of his infection but the fact that he passed through airport screening without triggering an alert. His only symptom at the time was a headache.
That is the epidemiological profile the Bundibugyo virus creates. Unlike the Zaire strain of Ebola that drove the 2014 West Africa outbreak and for which an approved vaccine now exists, Bundibugyo produces a somewhat longer incubation period and a case fatality rate of around 26 percent in the current DRC outbreak, lower than Zaire Ebola’s 40 to 70 percent in prior outbreaks. The lower rate is partly reassuring. It also means more people survive long enough to travel, and to board a flight in Kinshasa believing they are experiencing fatigue or a minor illness.
The outbreak began in Mongwalu health zone, northwest of Bunia in Ituri province in northeastern DRC, where Medecins Sans Frontieres teams received the first alerts on May 9 and 10, 2026, reporting a growing number of unexplained deaths in communities already stretched by years of armed conflict and displacement. The DRC Ministry of Health formally declared the outbreak on May 15. Two days later, the World Health Organization declared a Public Health Emergency of International Concern, its highest alert level. In the weeks since, the WHO has stated publicly that its own response is at about three or four on a scale of zero to ten.
In an assessment published this month, one month into the international response, the United Nations concluded that the scale-up remains insufficient. Ituri province now accounts for 1,020 of the DRC’s 1,118 confirmed cases, spread across 22 health zones. The outbreak has also reached North Kivu (95 cases, 11 health zones) and South Kivu (three cases from one health zone). Uganda has confirmed 20 laboratory-linked cases, including two deaths, all traced to cross-border movement from DRC. Uganda has reported no new cases since June 5.
There is a central reason the response has not replicated what ended the 2018–2020 DRC Ebola outbreak: there is no approved vaccine or treatment for Bundibugyo virus. The RVSV-ZEBOV vaccine that proved decisive in 2018 was engineered specifically against the Zaire strain and does not provide cross-protection. WHO is in emergency discussions about which candidate vaccines might be tested against Bundibugyo in accelerated clinical trials, but none have begun. MSF is building a 65-bed Ebola treatment centre in Ituri and has hundreds of staff in DRC and Uganda, providing isolation capacity and clinical care without the pharmacological tools that shrank the previous outbreak.
The arrival of the virus in France places that gap in its clearest context yet. European health systems have managed imported Ebola cases before; the United States, Spain, and the United Kingdom each treated returning workers during the 2014 outbreak. This is the first importation of the current Bundibugyo strain outside Africa. France’s health authorities say the risk of onward transmission is minimal at the viral load detected in the returning doctor, and the country’s infectious-disease isolation capacity has been substantially upgraded since 2014. The country’s hospital systems were already handling pressure from a heatwave that killed more than 150 people across France and Spain earlier this month, though specialized Ebola isolation wards operate outside the general hospital pathway.
The France case is the clearest illustration yet that an outbreak generating the worst first-month case numbers in Ebola history does not stay where it begins. Ituri is a province that receives little sustained international coverage outside moments of acute crisis; the region has had overlapping emergencies, including armed conflict, displacement, cholera, and measles outbreaks that stretched public health systems across central Africa, for years before this one. The contacts traced to the DRC doctor’s flight represent five people in isolation who had no particular connection to the DRC, no knowledge of where Ituri is, and no awareness that a virus declared a global health emergency in May had the capacity to sit beside them on an ordinary European flight.
The WHO has not stated a timeline for when the DRC outbreak might be brought under control. What it has said is that the current response, rated three or four on a scale of zero to ten, is not adequate to turn the curve. A vaccine trial that does not exist yet, a contact-tracing network still being built across 22 Ituri health zones, and a humanitarian response the United Nations has described as insufficient are the instruments being counted on. Until they work, the flight from Kinshasa to Paris will remain one of the ways the world receives its updates.