A quiet revolution is unfolding in transplant medicine—one that could dismantle one of its most entrenched burdens: lifelong dependence on anti-rejection drugs.
In a first-of-its-kind human trial, researchers at the University of Pittsburgh and UPMC have demonstrated that it may be possible to train the immune system to accept a transplanted liver as its own, eliminating the need for chronic immunosuppressive therapy in a subset of patients. The findings, published in Nature Communications, signal a potential paradigm shift in how organ transplantation is managed.
For decades, transplant recipients have been tethered to immunosuppressive drugs—powerful medications designed to prevent the body from attacking a foreign organ. These drugs are effective, but at a cost: increased vulnerability to infections, cancer, kidney damage, and metabolic disorders including diabetes. The burden of these immunosuppressive drugs side effects has long defined post-transplant life.
This breakthrough challenges that trade-off.
Engineering Tolerance Instead of Suppression
The approach is conceptually radical but biologically elegant. Instead of suppressing the immune system after transplantation, scientists attempt to educate it beforehand.
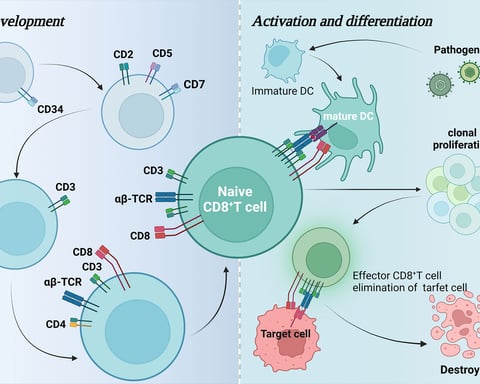
In the trial, researchers extracted immune cells—specifically monocytes—from liver donors and reprogrammed them into regulatory dendritic cells, or DCregs. These specialized cells are known to play a critical role in immune tolerance, essentially teaching the body to distinguish between harmful invaders and benign or beneficial tissue. The broader field of dendritic cell immunotherapy research has increasingly pointed to this strategy as a frontier in precision medicine.

“The idea is to teach immune cells in the recipient’s body to treat the donated liver fragment as familiar tissue, not an invader,” researchers explained.
Early Results, High Stakes
The trial remains small—just 13 participants—but the implications are outsized.
Eight patients were deemed eligible to attempt withdrawal from immunosuppressive drugs one year after surgery. Of those, four successfully discontinued the medications entirely. Three have remained drug-free for more than three years.
That translates to a 37.5 percent success rate among eligible participants—nearly triple the historical rate of about 13 percent in similar patients without such intervention.
Even more striking is what this represents conceptually. In transplant medicine, immune tolerance has long been described as the field’s “holy grail.” This study does not claim to have achieved it universally—but it edges closer than most previous attempts.
Why the Liver Is the Ideal Test Case
The liver is uniquely suited for such experimentation. Unlike other organs, it possesses a remarkable ability to regenerate. Living donors can give a portion of their liver, which then regrows in both donor and recipient.
This regenerative capacity has made liver transplantation a fertile ground for innovation. It also provides a relatively controlled setting to test immune tolerance strategies, particularly in living donor scenarios where timing and preparation are more predictable.

The Cost of Current Standard Care
The urgency behind this research is not theoretical. Long-term immunosuppression is associated with a cascade of complications.
Patients face elevated risks of opportunistic infections and malignancies. Kidney toxicity is common, often leading to secondary organ damage. Metabolic disorders—including hypertension and diabetes—are frequent consequences.
The possibility of eliminating—or even reducing—these drugs could dramatically improve both lifespan and quality of life.
Caution Beneath the Optimism
Despite the excitement, researchers are careful not to overstate the findings.
The study was not designed to prove definitive efficacy. Its sample size is small, and the results are preliminary. Larger, randomized controlled trials are already being proposed to validate the approach and refine patient selection criteria. Details of the clinical trial on immune tolerance in liver transplantation underscore the complexity and long-term ambition of this research.
Future iterations may also explore variations—such as using different immunosuppressive regimens initially, administering the engineered cells after surgery, or expanding the technique to organs beyond the liver.
“There are so many tantalizing paths we could take,” the researchers noted, emphasizing that collaboration across transplant centers will be key to scaling the science.
A Glimpse of Post-Drug Transplantation
What emerges from this study is not just a clinical advance but a conceptual pivot.
For half a century, transplant medicine has operated on a blunt principle: suppress the immune system to save the organ. This trial suggests a more refined future—one in which the immune system is not suppressed, but retrained.
It is a shift from pharmacology to immunological engineering, from chronic management to potential cure.
And if these early signals hold, the implications extend far beyond liver transplants.