
ST. LOUIS — For years, veterans in the waiting rooms of clinics across the country were handed two separate problems: a prescription for their weight, and a referral to addiction counseling they often could not reach. A growing body of research now suggests the first prescription may have been quietly addressing both.
A landmark study of 606,434 U.S. veterans with type 2 diabetes, published in March in The BMJ, found that those prescribed GLP-1 receptor agonists, including semaglutide-based medications sold under brand names Ozempic and Wegovy, were significantly less likely to develop a substance use disorder or, if they already had one, to overdose, be hospitalized, or die from it. Overdose events fell by 40 percent among users with existing addictions. Drug-related deaths dropped by half.
The researcher who led the study, Ziyad Al-Aly, a clinical epidemiologist at Washington University School of Medicine in St. Louis and chief of research at the VA Saint Louis Health Care System, offered an explanation for why the benefits extended across every substance his team studied, from alcohol and cocaine to nicotine and opioids. “GLP-1 drugs may quiet what I call ‘drug noise,'” Al-Aly said, “the relentless craving that drives addiction across substances.” The drugs appear to work not by targeting the chemistry of any one substance but by dampening the reward-system signals that make craving so persistent.
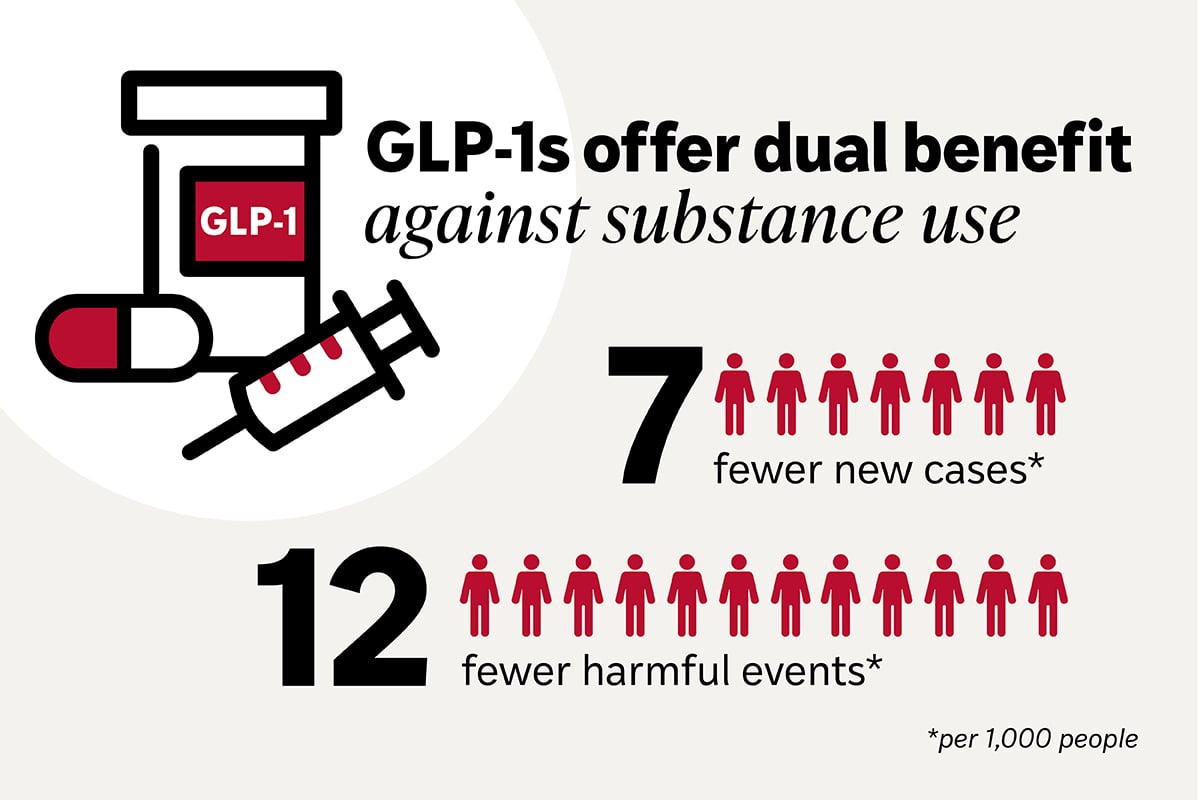
The study compared GLP-1 users against veterans taking SGLT2 inhibitors, a different class of diabetes medication, over three years. Among those without a baseline disorder, GLP-1 users were 14 percent less likely to develop any new substance use disorder, with the protective effect sharpest for opioids at 25 percent and for cocaine and nicotine at 20 percent each. Among veterans who already had a disorder, GLP-1 use was associated with 30 percent fewer emergency department visits and 25 percent fewer hospitalizations. Seven fewer veterans per 1,000 developed a new disorder; 12 fewer per 1,000 experienced a serious harm event.
The large-scale observational data were followed in May by the first rigorous placebo-controlled trial, published in The Lancet. The trial enrolled 108 adults with alcohol use disorder and comorbid obesity at Copenhagen University Hospital, randomizing them to either weekly semaglutide injections or a placebo for 26 weeks. The decrease in heavy drinking days was significantly larger in the semaglutide group. The drug’s number needed to treat for meaningful alcohol reduction came in at 4.3, substantially better than the 7 or higher recorded for naltrexone and acamprosate, the medications currently approved by the Food and Drug Administration for alcohol use disorder.
An earlier Phase 2 trial, published in JAMA Psychiatry in July 2025 by researchers at the Keck School of Medicine at the University of Southern California, found similar signals in a smaller sample of 48 adults, with semaglutide producing significantly lower weekly alcohol craving levels and greater reductions in heavy drinking days throughout the nine-week study. Among the 27 percent of participants who also smoked, the semaglutide group showed greater cigarette reduction, a finding consistent with GLP-1 researchers’ emerging hypothesis: the drug works on the brain’s reward system broadly, not on any single substance specifically.
The findings arrive as GLP-1 drugs are becoming more financially accessible. Medicare began covering the medications for seniors in July, extending treatment that had been out of reach for many older Americans. More than 30 clinical trials are now investigating semaglutide and related compounds for alcohol, nicotine, opioid, cocaine, and methamphetamine use disorders, with a Veterans Affairs Phase 3 trial focused on alcohol use disorder among the largest now enrolling.
The scale of the problem those trials are targeting is substantial. Roughly 46 million Americans have a substance use disorder, according to federal estimates, but only a fraction ever receive the pharmacological treatments that evidence supports. George Koob, director of NIH’s National Institute on Alcohol Abuse and Alcoholism, has described a more accessible and effective option for alcohol use disorder as a potential “gamechanger for closing the treatment gap.” Naltrexone, the first-line approved medication for alcohol use disorder, is prescribed to fewer than 10 percent of eligible patients.
Al-Aly has been measured in how he frames the implications. His data come from a population of veterans with diabetes, predominantly male and older, and he has said his study’s findings are not sufficient to justify replacing approved addiction treatments with GLP-1 drugs. It is not yet established whether the same effects would appear in younger populations, in women, or in people without diabetes who might eventually be prescribed the medications for addiction specifically. Some addiction specialists have cautioned against reading observational associations as a direct basis for off-label prescribing.
At the regulatory level, no GLP-1 drug has been approved for addiction treatment, and any such approval would require Phase 3 trial evidence that is not yet complete. The FDA has moved aggressively to restrict compounded GLP-1 formulations that spread during supply shortages, tightening control over which products reach patients. That effort has constrained access even for patients with straightforward diabetes or weight-management indications, let alone for addiction applications that have no approved pathway yet.
The drugs are not without side effects. A surge in poison control calls tied to GLP-1 drugs in recent months, most involving nausea, vomiting, and dosing errors with injectable formulations, prompted FDA warnings about labeling. Researchers testing semaglutide for addiction are monitoring those same effects in their trial populations, and the weight changes the drugs produce add a confounding variable that addiction researchers have not fully disentangled from the medications’ direct effects on craving.
The question the current evidence base cannot yet answer is whether GLP-1 drugs will show the same protective effects in people whose addiction exists without the obesity or diabetes that currently qualify them for these medications. That population represents the majority of Americans with substance use disorders. The mechanism that makes these drugs intriguing for addiction treatment is also the source of the uncertainty: it is not yet clear how much of the effect comes from metabolic changes, from appetite suppression, or from something in the brain’s dopamine pathways that researchers have only begun to map. That is what the trials still running are designed to find out.