
EDINBURGH — When patients leave the hospital after a lacunar stroke, they leave carrying a familiar prescription: aspirin. A study published Thursday in Circulation suggests that prescription has spent decades addressing a cause that was never actually there.
Researchers at the University of Edinburgh found that lacunar ischemic stroke, which accounts for roughly a quarter of all ischemic strokes in the United Kingdom, is not driven by fatty deposits building up inside arteries, as has long been assumed. The real mechanism appears to be damage and abnormal widening in the brain’s own small blood vessels, deep within the tissue.
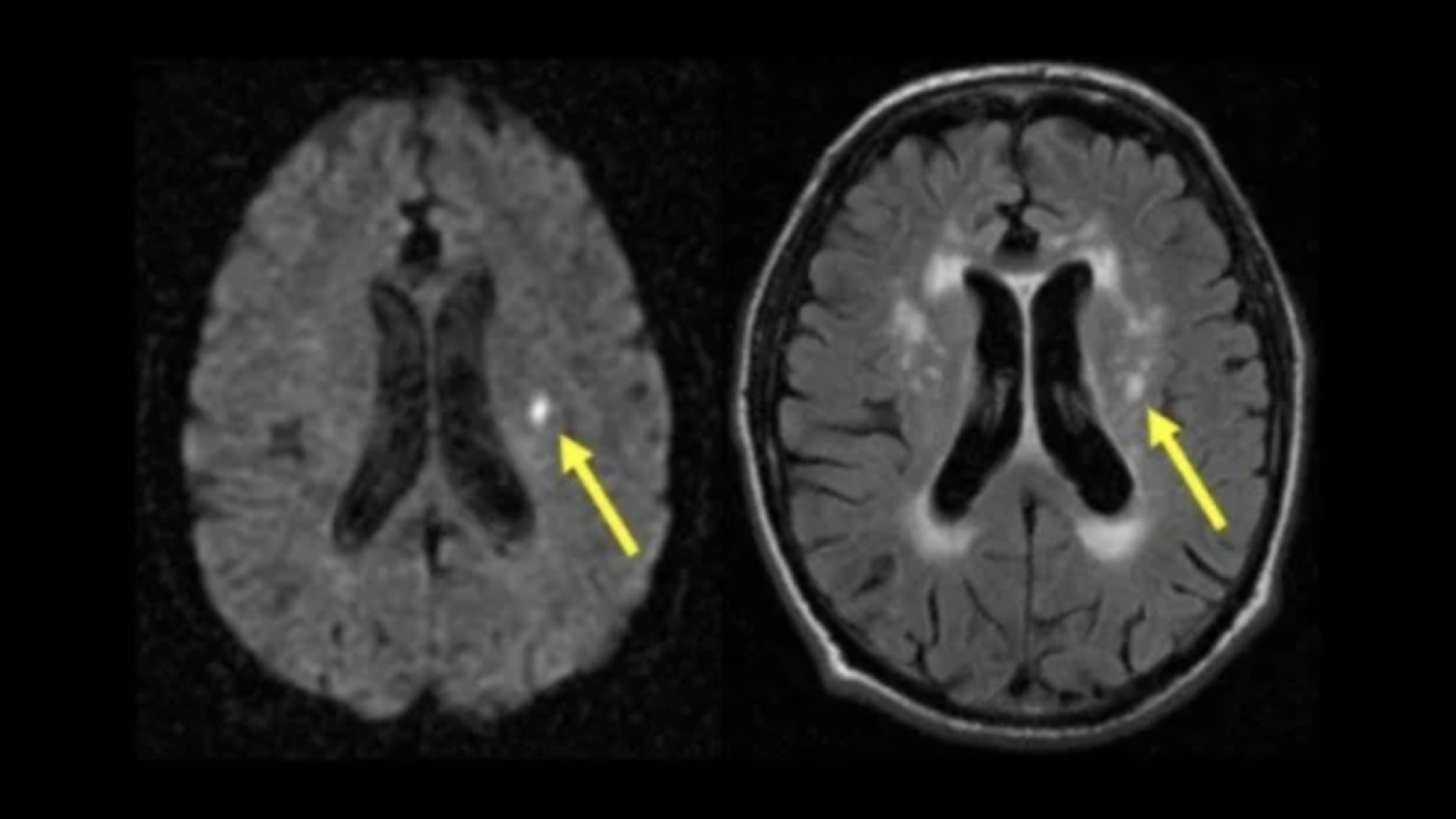
The study, led by Professor Joanna Wardlaw at Edinburgh’s Institute for Neuroscience and Cardiovascular Disease, followed 229 patients using MRI brain scans at the time of stroke and again one year later. Patients who showed evidence of arterial widening in the brain were more than four times as likely to have experienced a lacunar stroke as those who had not. By contrast, narrowing of larger arteries by fatty plaque buildup showed no significant connection to this type of stroke at all.
The distinction matters because antiplatelet drugs like aspirin work by preventing clots from forming on fatty plaques in larger arteries. If the condition underlying lacunar stroke is not atherosclerotic plaque but damage to the small vessel network, then aspirin is not correcting anything. It is treating something that is not there.
That may explain a stubborn clinical puzzle. Trials have repeatedly found antiplatelet therapy is less effective in lacunar stroke than in other ischemic stroke types. In the Secondary Prevention of Small Subcortical Strokes trial, adding clopidogrel to aspirin did not reduce recurrent stroke in lacunar stroke patients and was associated with increased bleeding and death. The patients followed the treatment. The treatment did not follow the disease.

The Edinburgh study drew patients from the Mild Stroke Study 3, a prospective cohort recruited through Edinburgh stroke services between 2018 and 2021. Despite receiving standard preventive treatment, more than a quarter of participants developed new silent strokes within the follow-up year. Those are small brain injuries with no obvious symptoms that accumulate gradually, affecting memory, processing speed, and gait over time.
The mechanism the research identified involves what clinicians call dolichoectasia: a condition in which brain arteries become widened, elongated, and sometimes distorted in shape. In the brain’s small vessel network, this distortion appears to damage vessel walls and disrupt blood flow in ways that can eventually trigger a lacunar infarct. The study found a particularly strong association between dolichoectasia of the basilar artery, a major blood supply route to the back of the brain, and lacunar stroke.
“This study provides strong evidence that lacunar stroke is not caused by fatty blockage of larger arteries, but by disease of the small vessels within the brain itself,” Wardlaw said. Recognizing that distinction, she noted, explains why antiplatelet drugs are not effective for this type of stroke and points toward the urgent need for therapies targeting microvascular damage directly. The full findings were published in Circulation on Thursday.
The research is already informing one such attempt. The LACunar Intervention Trial 3, known as LACI-3, is now testing cilostazol and isosorbide mononitrate across 38 centers in the United Kingdom, aiming to recruit 1,300 lacunar stroke patients over 18 months. Both drugs are designed to act on the blood vessel wall directly, rather than on clotting, which is the mechanism aspirin targets. Results are not yet available.
The broader picture emerging from small vessel disease research points to dysfunction in the blood-brain barrier and microvascular inflammation as key drivers of lacunar stroke, processes aspirin was never designed to address. The Edinburgh team described the new LACI-3 trial as testing drugs that work through a fundamentally different pathway, one intended to protect the small vessel endothelium rather than prevent clotting on plaque that may not be the primary problem.
The study has one acknowledged limitation that carries weight. All 229 participants were drawn from stroke services in Edinburgh alone. Whether the findings hold across broader geographic, demographic, and ethnic populations remains untested. The authors called for larger multi-center studies to confirm the results. Until then, the conclusions apply with confidence to a specific population, which is not the group that bears the heaviest global stroke burden.
What the Edinburgh study cannot yet answer is when vessel-targeted therapies might reach clinical guidelines, or whether the LACI-3 results will be sufficient to shift standard prescribing at scale. For now, thousands of lacunar stroke patients leave hospital each year with prescriptions written against the wrong theory of their disease. That gap between the current evidence and what is handed to patients is the most urgent question the Wardlaw team has now opened.