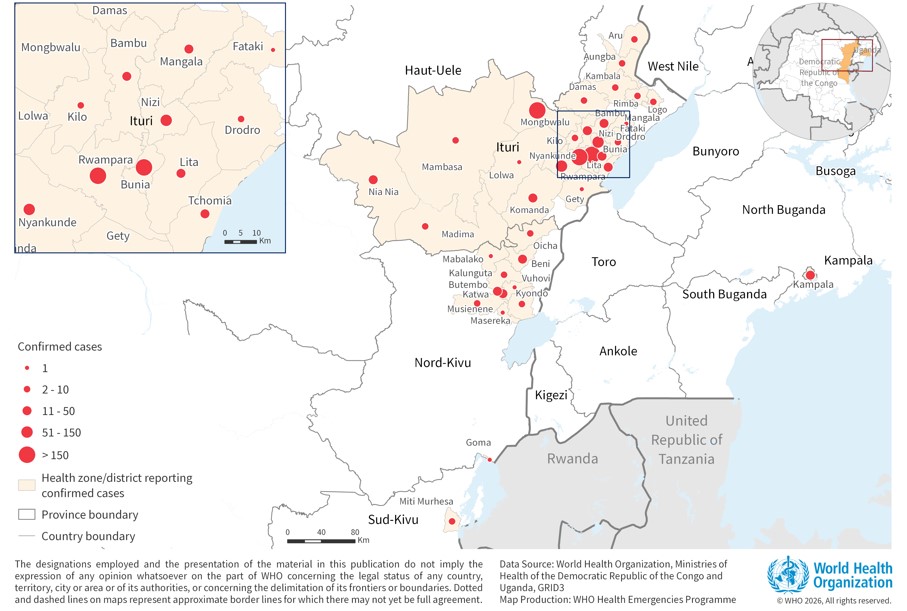
KINSHASA — The Ebola outbreak that has killed 702 people in the Democratic Republic of the Congo reached Tshopo province Saturday — whose capital, Kisangani, is one of the country’s largest cities and its main river transport hub in the northeast. Health Minister Samuel Roger Kamba confirmed Friday that the virus had spread to Tshopo and Haut-Uele, a second new province bordering South Sudan, bringing the total under enhanced surveillance to five.
The DRC’s Ministry of Communication and Media reported 1,926 confirmed cases in total, including 702 deaths and 318 recoveries. In Tshopo, four cases have been detected, two of them fatal. Haut-Uele has recorded one death. Investigators believe both sets of cases were imported from Niania in Ituri province — the outbreak’s epicenter — pointing to human movement as the mechanism of spread rather than independent new chains of transmission. That distinction matters for containment. For now, it holds.
A senior World Health Organization official has warned that four out of five newly confirmed Ebola cases in the DRC have no known link to existing patients, and that the true scale of the outbreak could be two to four times larger than official data indicate. At two months into an active outbreak, that ratio signals that contact tracing is not keeping pace with transmission.
The WHO declared the Ebola epidemic in the DRC and Uganda a public health emergency of international concern on May 17, citing high risk of regional spread. Uganda has confirmed cases and deaths. France confirmed a case in a physician who returned from a medical mission in the DRC — the first Ebola case in Europe from the current outbreak — with no secondary infections reported.
Tshopo’s significance is partly geographic, partly logistical. Kisangani sits at the confluence of the Congo River and the Lualaba, making it a major junction for waterborne movement across a region where road infrastructure is limited and populations are highly mobile. A sustained transmission chain in Kisangani — as distinct from the imported cases detected so far — would represent a different containment problem from the rural health-zone response that has structured the Ituri effort. DRC health authorities have placed the province under enhanced monitoring rather than declaring a local outbreak. That designation could shift quickly.
Haut-Uele introduces a different variable. The province’s northern border with South Sudan and the Central African Republic brings the outbreak within geographic reach of countries whose own health system capacity would be tested by any cross-border spread.
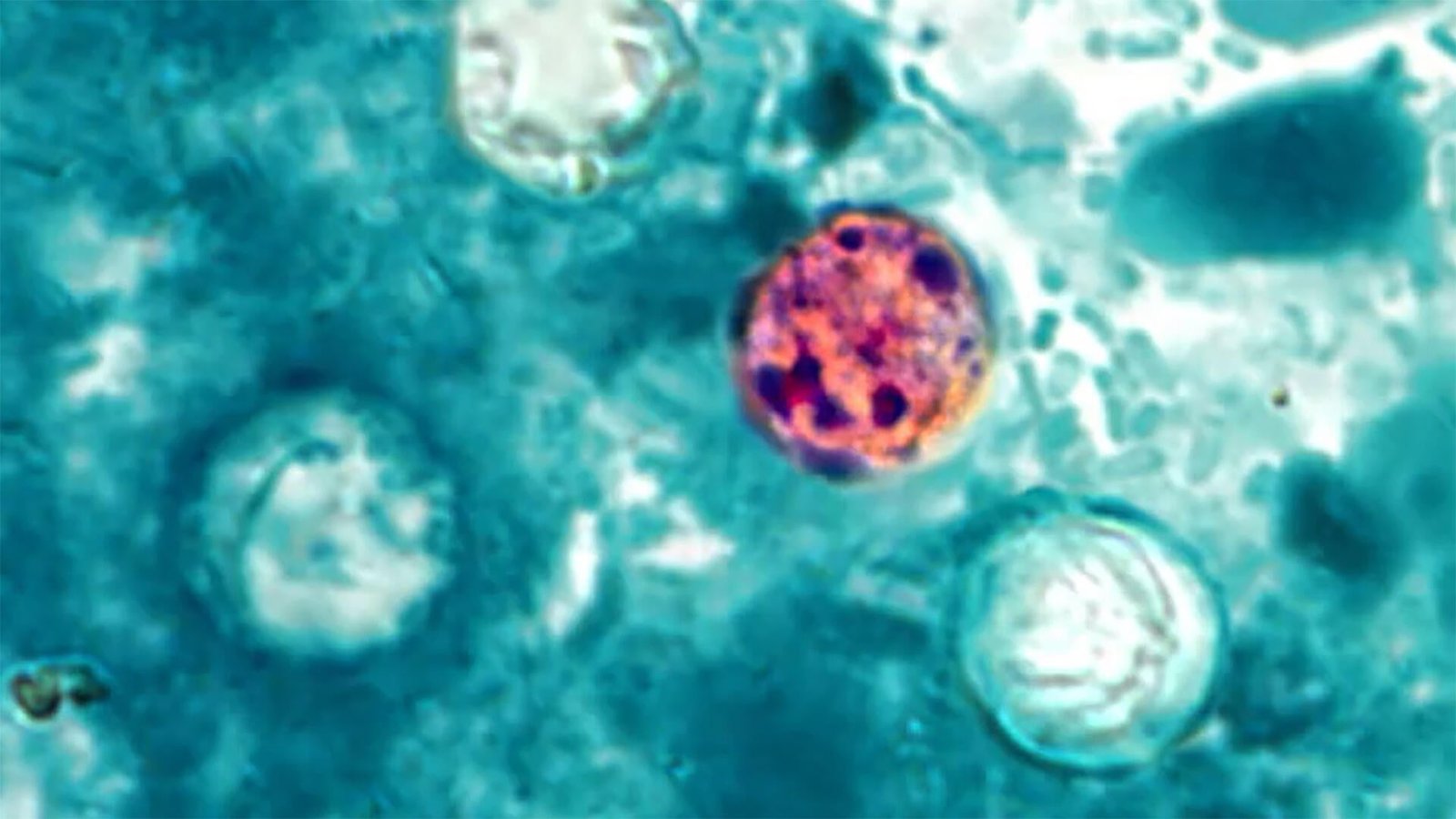
The outbreak is Congo’s 17th involving Ebola. It is caused by the Bundibugyo ebolavirus — a variant for which no approved vaccine or treatment exists, complicating the response compared to earlier DRC outbreaks caused by the Zaire ebolavirus, for which effective vaccines are available. Scientists launched the first clinical trial for Bundibugyo-specific treatments earlier this month, but no approved countermeasure is available to the current response.
The CDC has characterized this as the fastest-growing Ebola epidemic on record in Africa, surpassing 1,000 confirmed cases within 40 days of response activation — a pace that took 235 days during the 2018 North Kivu outbreak. Response operations have faced sustained obstacles: attacks on health centers, funding constraints, community mistrust of official health messaging, and reported payment delays for outbreak responders. Dr. Biensi Kano, a member of the epidemiological surveillance committee in Bunia, said publicly that workers had been demanding payment since the outbreak was declared — a pattern that has interrupted contact tracing at critical moments in previous DRC outbreaks.
India’s airlift of medical supplies to support Congo’s Ebola response has provided additional resource coverage, but structural funding constraints and the geographic spread of the outbreak have not been resolved by external assistance alone.
Whether Tshopo and Haut-Uele develop into active local transmission zones or remain isolated imported events is the operational question that will define whether the outbreak has fundamentally changed in character. The official classification — enhanced monitoring — implies sustained local transmission has not yet begun. What the current surveillance data cannot answer is how long that framing holds, and whether the case count captures what is actually happening in provinces where health infrastructure is thin and case detection is incomplete.
That is the gap the current figures do not close.