
LONDON – For patients with relapsed multiple myeloma in Britain, the appearance of a fever within hours of receiving a cancer immunotherapy can mean one thing: the treatment that was supposed to save them has triggered an immune overreaction violent enough to land them in intensive care. It is called cytokine release syndrome, and it affects somewhere between 60 and 80 per cent of patients receiving some of the most effective cancer therapies now available. There is, at present, no drug approved anywhere in the world to prevent it.
That is the problem a small AIM-listed Irish company, Poolbeg Pharma (LSE: POLB), has spent three years trying to solve. This week, its lead experimental drug – an oral p38 MAPK inhibitor called POLB 001 – cleared the last bureaucratic hurdle and began recruiting the first patients at its clinical trial site in London, with interim results expected before September.
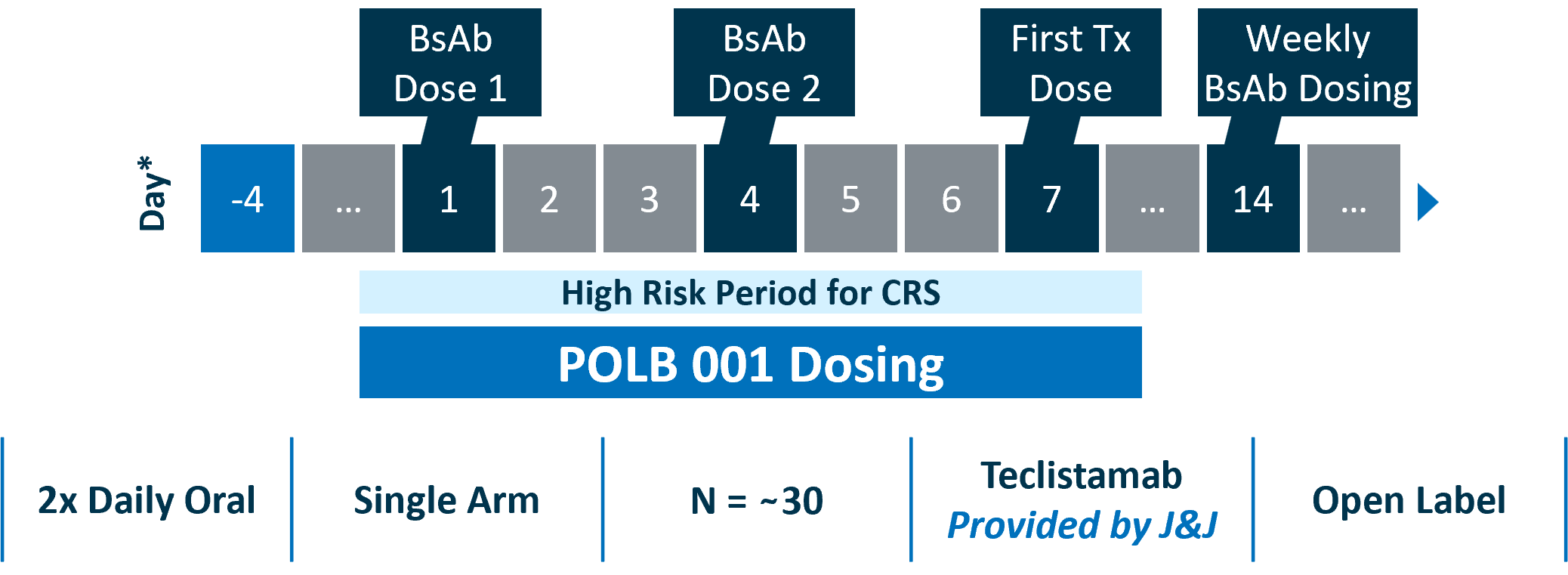
The trial, named TOPICAL, is enrolling approximately 30 patients with relapsed or refractory multiple myeloma at six sites across the National Health Service: The Christie NHS Foundation Trust in Manchester, The Royal Marsden, University College London Hospitals, University Hospitals Birmingham, NHS Lothian in Edinburgh, and Royal Stoke University Hospital. Patients in the single-arm study are receiving teclistamab, a bispecific antibody sold by Johnson & Johnson under the brand name Tecvayli. Johnson & Johnson is supplying the drug for the trial at no cost to Poolbeg – a detail that speaks to the commercial interest already circling the programme.
The therapy Poolbeg is testing is not a treatment for cytokine release syndrome. It is a prevention. That distinction matters enormously to the oncologists running the trial and, if the drug works, to the architecture of modern cancer care. Cytokine release syndrome is currently managed reactively – with injectable tocilizumab and corticosteroids administered after the storm has already broken. That approach works, more or less, but it requires patients to be treated in specialist cancer centres equipped to handle the emergency. The consequence is that bispecific antibodies and CAR-T cell therapies, which have transformed outcomes for blood cancer patients, remain largely unavailable in community hospitals.
Dr Emma Searle at The Christie, who is leading the TOPICAL study, is working from a hypothesis that shifting CRS management from reactive to preventative would allow these treatments to reach patients who currently cannot access them. The argument is structural: if you eliminate the emergency, you eliminate the constraint on where the treatment can be given.
Preclinical data presented this past week at the European Hematology Association Congress in Stockholm added texture to that hypothesis. Two posters, one from Poolbeg and one from the University of Manchester, showed that POLB 001 reduced key CRS-associated cytokines – including TNF, IFN-gamma, and IL-6 – in both in vitro and in vivo models without impairing the bispecific antibody’s ability to kill tumour cells. That last point is not trivial. An anti-inflammatory agent that suppresses the immune storm but also blunts the anti-cancer effect would be clinically useless.
The Manchester data also raised a secondary possibility: that POLB 001 might enhance the effectiveness of azacitidine, a first-line treatment for acute myeloid leukaemia, in elderly patients – a potential second indication the company has not yet committed to developing.
The regulatory runway has been cleared on both sides of the Atlantic. The UK Medicines and Healthcare products Regulatory Agency granted clinical trial authorisation for TOPICAL in April. In May, Poolbeg disclosed that the US Food and Drug Administration had broadly aligned with its development plan, including agreement on the primary endpoint for a future Phase III trial. The FDA also granted Orphan Drug Designation to POLB 001, which would provide seven years of US market exclusivity after any eventual approval.
None of this guarantees the drug works in patients. Phase I trials enrolling 30 subjects are designed primarily to confirm safety and signal early efficacy, not to establish clinical proof. The interim data expected this summer will be scrutinised closely by prospective licensing partners, and Poolbeg has been explicit that its commercial strategy is not to bring POLB 001 to market itself but to partner with a larger pharmaceutical company at a clinical inflection point. The company has put the addressable US market for a CRS preventative at over ten billion dollars, a figure derived from independent payer research by Acumetis Global and one that will face its own scrutiny once trial data become available.
What the company can say today is that POLB 001 has a plausible mechanism, a clean preclinical record, and six NHS sites actively recruiting patients – a wider trial footprint than most early-phase oncology studies achieve. Liam Tremble, Poolbeg’s Principal Scientist, said the EHA data reinforced the company’s belief that the drug could play a meaningful role in improving both the safety and accessibility of cancer immunotherapies. He added that the company looks forward to sharing interim data from the TOPICAL trial in multiple myeloma patients later this summer.
What neither Tremble nor the company can say yet is whether the data will show what the preclinical models suggested. For the patients currently being enrolled at The Christie and five other NHS sites, that answer is still weeks away.
GSK’s $10.6 billion acquisition of Nuvalent in June underscored how urgently major pharmaceutical companies are seeking to expand their oncology portfolios. Chinese biotech firms struck $60 billion in outbound licensing deals with Western pharma this year, further tightening competition in the same cancer-treatment verticals where Poolbeg is operating. Earlier research showing the thymus as a hidden driver of cancer outcomes pointed in the same direction: the field is searching, urgently, for ways to make immunotherapy work for more patients, not fewer.