
PARIS – The first Ebola patient in France arrived quietly, isolating himself before French health authorities had confirmed the diagnosis. The doctor had returned from a humanitarian mission in the Democratic Republic of the Congo, where he had been treating patients with the virus that would follow him home.
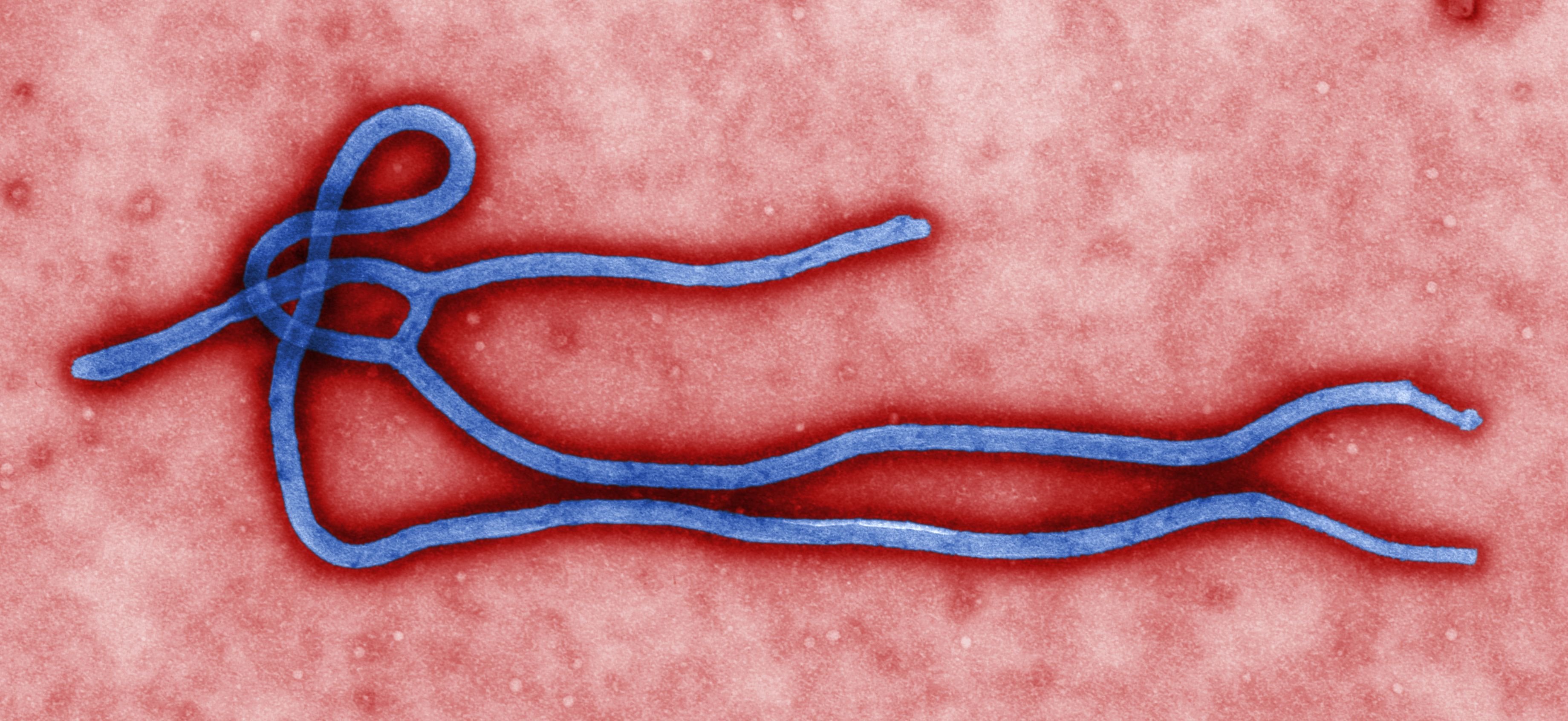
On Wednesday, France’s Health Ministry confirmed what he already suspected: he had tested positive for Bundibugyo virus disease, making him the first person to carry Ebola out of Africa during an outbreak that has been spreading faster than any in recorded history, Al Jazeera reported.
The case is a threshold moment. Since the epidemic was identified in the DRC’s northeastern Ituri Province in early May, it has killed 291 people and infected 1,118, according to DRC Ministry of Health figures through June 24. The World Health Organization, which declared the outbreak a Public Health Emergency of International Concern on May 17, has described the speed of transmission as unprecedented for the Bundibugyo strain.
The Bundibugyo virus is not the Zaire ebolavirus that drove the 2014 West Africa epidemic and the subsequent development of the rVSV-ZEBOV vaccine. That vaccine does not cross-protect against Bundibugyo, and in May the WHO recommended against its use in this outbreak. There is no approved vaccine for the Bundibugyo strain and no approved specific treatment. Available therapies, including the antiviral remdesivir and two experimental monoclonal antibody drugs, MBP-134 and maftivimab, are supportive rather than curative. The Coalition for Epidemic Preparedness Innovations announced in June it was funding three vaccine candidates: a $50 million contract with Moderna, $8.6 million to the University of Oxford, and $3.2 million to IAVI. None will arrive in time to help the people who are sick today.
The geography of the outbreak explains why containment has been so difficult. Ituri Province accounts for 1,020 of the 1,118 confirmed cases and sits in a part of northeastern DRC affected by persistent armed conflict and severely limited health infrastructure. North Kivu, where 95 cases have been confirmed across 11 health zones, borders Uganda. Transmission has crossed into Uganda, and the WHO is coordinating cross-border preparedness measures. By this week, the outbreak had reached 34 health zones across three DRC provinces.
The French doctor’s case is the second time this outbreak has reached Europe. In May, an American citizen was medically evacuated to Germany for treatment under controlled conditions. France’s case differs in one critical respect: it was not a medical evacuation. The doctor had been working in the affected region, carried exposure risk, and returned on a scheduled journey. His decision to self-isolate on arrival and seek testing quickly was what French authorities credited as the difference between a contained import and a potential transmission chain.
France’s Health Ministry placed 21-day monitoring requirements on all contacts since the doctor’s return. It did not disclose the number of contacts or the circumstances of his travel, citing patient confidentiality. An epidemiological investigation was ongoing.
For healthcare workers in the outbreak zone, the France case illustrated the weight the response places on them. The DRC Ministry of Health has reported multiple infections among health workers in Ituri Province, a characteristic of the Bundibugyo strain, which spreads through direct contact with bodily fluids and demands strict protective protocols in clinical settings that often lack them. The doctor who brought it to France was himself providing that care.
The UN warned this week that the outbreak was outpacing response, citing three specific gaps: insufficient contact tracing, inadequate treatment capacity, and failures in safe burial practices. More than a month in, frontline responders had expanded care at unprecedented speed, the assessment noted, but the basic infrastructure of epidemic control, knowing who has been exposed to whom, was not keeping pace with the rate at which new cases were appearing.
A continent whose hospital systems were strained to saturation point by a record heatwave this week now receives a different kind of alert from its health authorities. The France case will not become a European epidemic if isolation holds, contacts are tracked, and the single imported case does not become a chain. In Ituri Province, those same conditions have not held, which is how the 1,118 got to 1,118.
What nobody in Paris, Geneva, or Kinshasa could confirm on Friday was whether the doctor’s contact list was complete. Or whether any of the three vaccine programs would produce a viable candidate before the DRC outbreak reaches the size at which epidemic momentum becomes self-sustaining. What they could confirm was that the number of cases in Ituri Province was still rising.