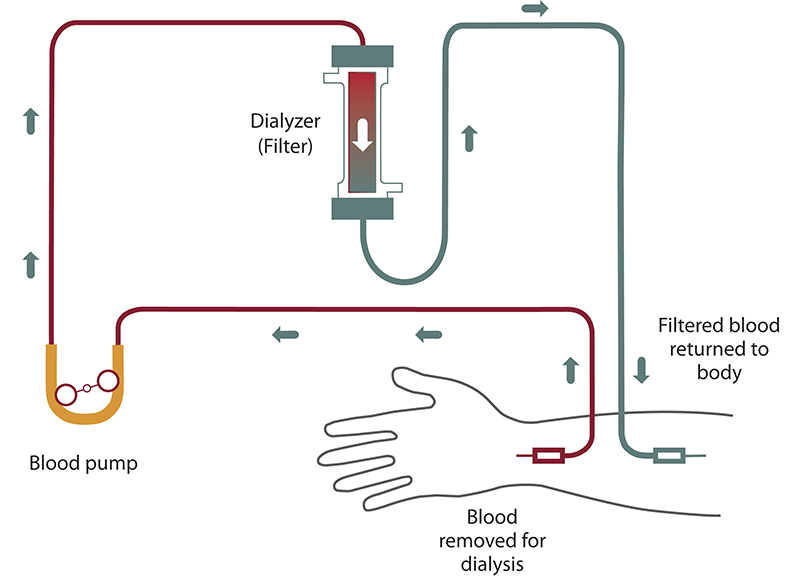

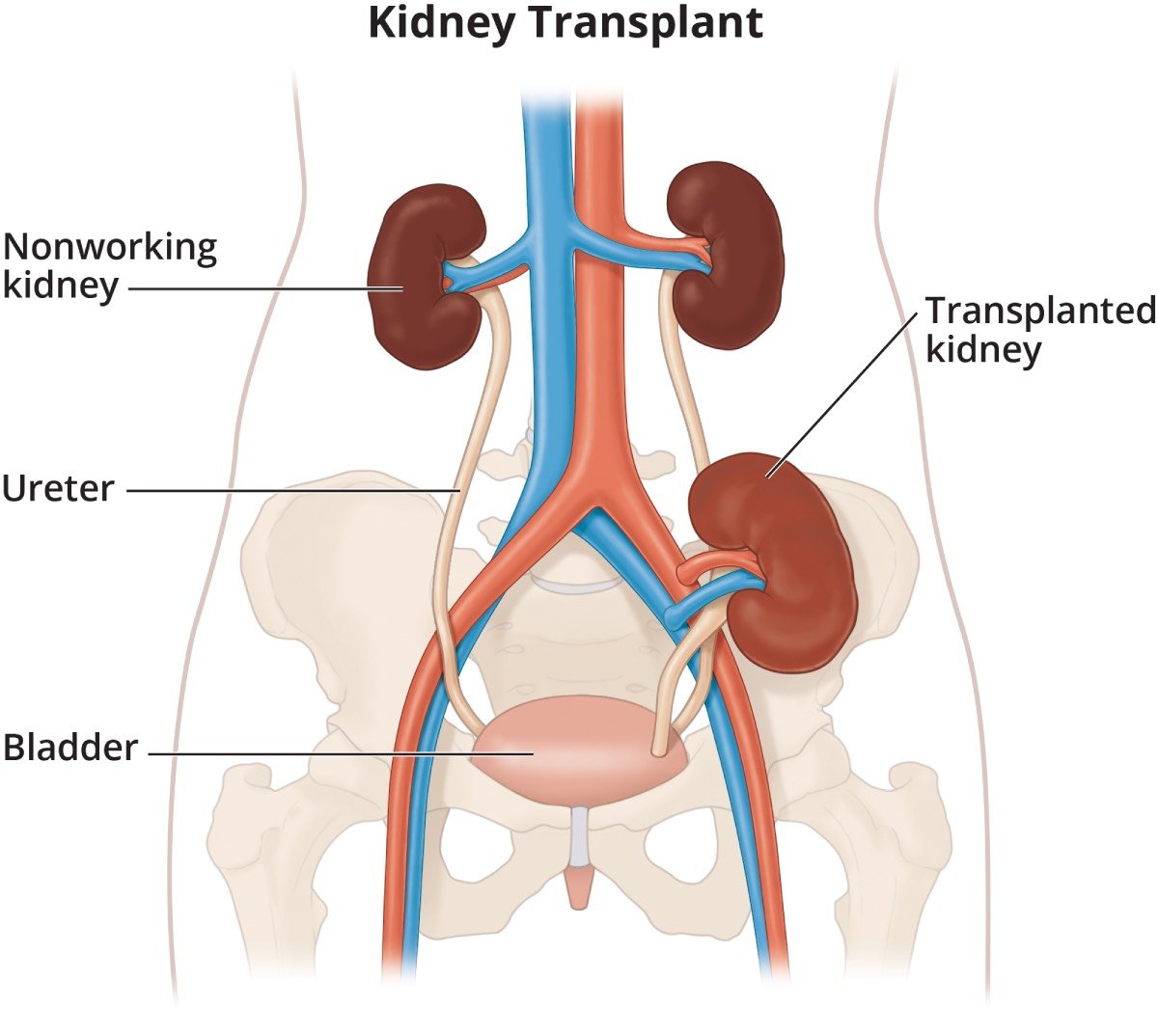
NEW YORK — For the roughly 100,000 Americans who begin dialysis each year, a kidney transplant is more than a better treatment. It is the only one that can fully reverse what kidney failure takes. It extends life, on average, by more than a decade, and it frees patients from the machines that substitute, imperfectly, for what two failing organs once did without thought. The path to getting one starts with a referral. A large new study found that for nearly half of all referred patients, that is also where the path ends.
Research published June 20 in the Journal of the American Society of Nephrology traced 720,348 patients referred for kidney transplantation across the United States between 2014 and 2025, one of the most comprehensive examinations yet of how the evaluation process actually unfolds in clinical practice. The numbers were direct: 48 percent of referred patients never initiated their evaluation, and only 19 percent completed the process and reached the transplant waitlist. What separated those who advanced from those who disappeared was not purely their medical condition. It was where they lived, what language they spoke, whether they were married, and which transplant center was treating them.
“Which transplant center you go to, where you live, and even whether you are married all appear to influence your chances of moving forward to the waitlist for a new kidney,” said Dr. Conor B. Donnelly, the study’s lead author and an internist at NYU Grossman School of Medicine. Patients facing the highest barriers included unmarried individuals, those with severe obesity, rural residents, Spanish speakers, lower-income patients, and older adults. Those referred to smaller programs or facilities in the South fared measurably worse at every stage than patients who reached larger, better-resourced centers.
The transplant evaluation is not a single visit. It involves medical assessments spread across multiple appointments, including blood work, chest imaging, cancer screenings, and cardiac testing, all of which continue alongside ongoing dialysis treatment. In the United States, dialysis typically means three clinic sessions a week. For patients who lack reliable transportation, cannot afford time off work, live hours from their nearest transplant center, or are navigating a healthcare system in a language other than English, sustaining that schedule over months becomes a barrier in its own right. The evaluation process was designed with a defensible medical rationale: organs are scarce, and centers are obligated to place them where they are most likely to produce good outcomes. The NYU study reveals, with unusual precision, who the design filters out before that determination is ever made.
More than 37 million Americans have chronic kidney disease, according to the Centers for Disease Control and Prevention, most of them undiagnosed until the disease is advanced. For those whose kidneys fail entirely, dialysis keeps them alive but at an enormous cost in time, physical burden, and long-term survival. Mortality rates for Americans on dialysis are higher than those of many cancers. A successful transplant cuts that risk substantially and, in patients under 70, typically adds years of active life. Efforts to close similar gaps in preventive care, including recent moves to extend colorectal cancer screening to younger adults, have repeatedly shown that eligibility alone does not change outcomes unless the eligible can actually reach and navigate the system designed for them.
The research team reached its conclusions using Epic Cosmos, a database aggregating electronic health records from more than 300 million patients across 1,850-plus hospitals, including records from roughly one-third of all U.S. transplant centers. The scale allowed the team to follow individual patients through each discrete stage of the evaluation pipeline in ways that previous research, typically limited to single-center data or national registry snapshots, had not been able to do. Co-senior authors Dr. Allan B. Massie and Dr. Michal A. Mankowski, both affiliated with NYU Langone Health, have previously examined how social factors shape transplant access.
What the study tracks but cannot yet explain is whether these dropout rates have been improving or worsening across the 2014-to-2025 window the researchers examined. The geographic and facility-level differences they identified suggest that some programs move referred patients through evaluation at meaningfully higher rates than others. What those centers do differently, whether patient navigators, transportation assistance, or expanded language services account for the gap, has not yet been studied at this scale.
Related research this year has found similar dynamics in other specialties. An Oxford study published in The Lancet Digital Health used 5.6 million patient records to show that most statin-eligible adults are not currently receiving cholesterol-lowering medications, in part because risk communication and care access do not reliably reach those who need them. Across specialties, large health records studies are producing a consistent finding: institutional barriers, not disease severity alone, shape who receives the treatments with the largest potential benefits.
Organ donation rates have risen in the United States in recent years, and allocation policy has been revised to widen access for patients historically disadvantaged by earlier systems. Those changes reach only the patients who make it far enough to be listed. The NYU study’s core finding, that nearly half of all referred patients never begin their evaluation, suggests the more consequential gap may not be in what happens after listing but in what happens in the months between a referral and the first appointment, months that, for half of those referred, never arrive.