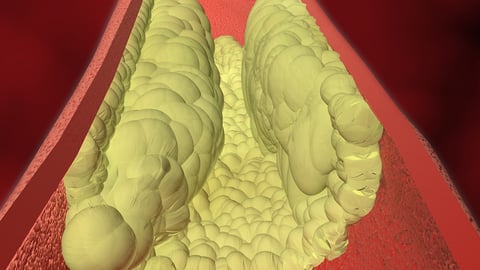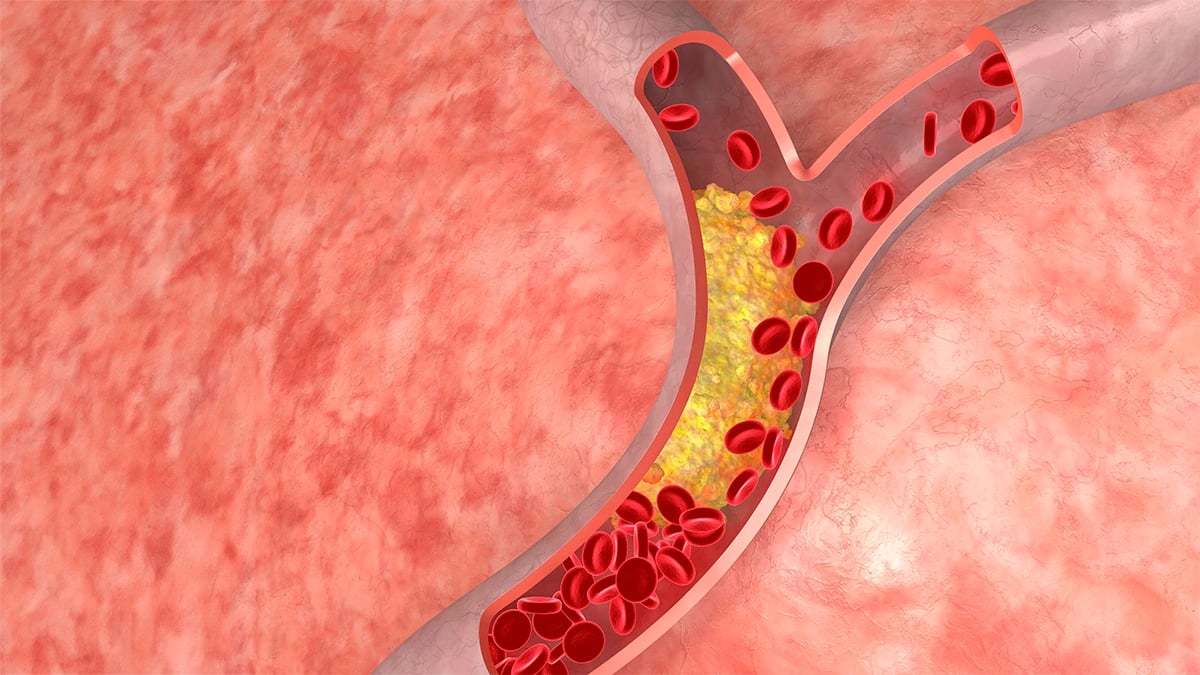

LONDON — For years, the fear of muscle pain and weakness has kept millions of patients from taking statins, the cholesterol-lowering drugs that cardiologists consider among the most effective tools in preventing heart attacks and strokes. A new calculator developed at the University of Oxford now offers what clinical medicine has never provided for those patients: a personal estimate of their actual risk, derived from the health records of 5.6 million people in England.
The tool, called STRATIFY-StatinMD, is described in a paper published Thursday in The Lancet Digital Health. It draws on 22 individual health factors to estimate a patient’s likelihood of developing a serious muscle disorder, the most feared among statin side effects, over a ten-year period. The headline finding: for more than 98 per cent of patients considered eligible for statin therapy, that risk is minimal.
Dr. Ting Cai, the study’s lead author and a researcher in Oxford’s Nuffield Department of Primary Care Health Sciences, said the gap between perceived and actual risk had driven the work from the start. “Serious muscle disorders are one of the most widely discussed concerns about statins, but our findings suggest that the risk is very low for the vast majority of people who may benefit from treatment,” she said.
That gap has consequences. More than 60 per cent of people considered eligible for statin therapy in England are not currently taking it. Cardiovascular disease remains the leading cause of death in the United Kingdom, responsible for roughly 160,000 deaths each year, and statins remain among the most rigorously tested means of reducing that toll. The perception of side-effect risk, rather than any lack of evidence for the drugs’ benefit, appears to be a significant driver of the treatment gap.
The muscle disorders statins can cause, including rhabdomyolysis and myopathy, are real but rare. In most patients, the more common complaint is mild and transient muscle aching that resolves when the drug is stopped or the dose adjusted. The serious variants, which involve genuine muscle fibre breakdown, occur far less often. Prior research had never provided a reliable way to distinguish in advance who was at elevated risk. STRATIFY-StatinMD was built to address that absence.
To build the tool, Dr. Cai’s team drew on a derivation dataset of 1.7 million primary care patients in England, then validated its predictions against a separate cohort of 3.9 million, one of the largest validation sets ever assembled for a pharmacological risk calculator. The twenty-two input factors span a patient’s age, existing conditions such as kidney disease or thyroid dysfunction, body mass index, and concurrent medications known to interact with statins.

James Sheppard, a senior author on the paper, said the study fills a gap that has long troubled clinicians trying to have balanced conversations with patients. “Treatment decisions are often based on estimates of a person’s future cardiovascular risk, but much less information is available about their individual risk of adverse outcomes,” he said. The asymmetry means patients often hear detailed statistics about heart attack risk reduction but receive little comparable data about what statin intolerance would actually mean for someone with their particular health profile.
Constantinos Koshiaris, another member of the Oxford team, framed the finding as a question of fairness in clinical reasoning. “Clinical decisions are often based on estimates of potential benefit, but understanding potential harms is equally important,” he said.
Evidence-based risk communication has emerged as a recurring challenge in preventive medicine. A recent Lancet review examining safety data from mRNA therapies similarly found that serious adverse outcomes were rarer than public perception suggested, pointing to a systemic difficulty in translating population-level statistics into individual clinical conversations.
At the population level, the stakes of treatment gaps are hard to overstate. Policymakers have drawn similar lessons from the recent expansion of colorectal cancer screening to younger age groups, where preventive programmes only deliver their statistical benefit when eligible individuals actually participate. The STRATIFY-StatinMD model is built on the same logic: if patients can see a personalised risk estimate rather than a population average, they may reach different decisions about their treatment.
The tool is currently available through Oxford University Innovation, the university’s commercialisation arm, intended initially for research and academic applications. What that means for the general practitioners managing the millions of statin-eligible adults in England who are not yet on treatment remains an open question. No timeline has been announced for review by the National Institute for Health and Care Excellence or for incorporation into NHS clinical guidelines.
The research was funded by the British Heart Foundation, the Wellcome Trust, the Royal Society, and the National Institute for Health and Care Research. Dr. Jennifer Hirst, Brian Nicholson, Richard McManus and F.D. Richard Hobbs of Oxford’s Nuffield Department are among the co-authors.
Statins, first approved for clinical use in the late 1980s, work by inhibiting an enzyme in the liver that produces low-density lipoprotein cholesterol. They are among the most prescribed drugs in the world, and the evidence for their benefit in patients at elevated cardiovascular risk is not seriously contested in the medical literature. What has always been harder to establish is whether the patients who refuse statins or abandon them after an initial prescription have an accurate sense of the risk they are weighing.
The answer from 5.6 million English primary care records, published in one of medicine’s most respected journals, is largely that they do not. For the researchers at Oxford, and for the clinicians who may eventually use their calculator, the harder problem is closing the distance between what the data now shows and what patients believe when they sit across from their doctor and consider whether a daily pill is worth the worry.