OMAHA — For 42 days, eighteen Americans lived in isolation rooms inside Nebraska Medicine’s quarantine and biocontainment facilities in Omaha, their release date governed by the maximum incubation period of one of the world’s most dangerous viruses. One of them, a physician, had initially tested positive for Andes hantavirus and been placed in a room designed for the world’s most lethal pathogens. On Monday, the last of the eighteen walked out.
The U.S. Department of Health and Human Services formally announced the conclusion of the federal hantavirus response on Monday, and the Centers for Disease Control and Prevention officially closed out the event on Wednesday, more than six weeks after the first Americans were evacuated from the MV Hondius following a shipboard outbreak that killed three people. The CDC said it had completed the 42-day monitoring period for all U.S. citizens identified as having potential exposure to the Andes virus, and that everyone had returned home safe. Of the 18 Americans monitored across Nebraska Medicine’s National Quarantine Unit and Emory University Hospital in Atlanta, not one developed hantavirus disease.
The outbreak traced to the MV Hondius, a polar-class expedition vessel operated by Oceanwide Expeditions returning from a South Atlantic voyage between South America and West Africa. When passengers began developing severe respiratory symptoms consistent with Andes hantavirus infection, the ship diverted to Spain’s Canary Islands. More than 120 people were evacuated from the vessel in early May, including the 18 Americans subsequently flown to Nebraska. Eastern Herald covered the outbreak from the moment the Hondius went into emergency quarantine off the Canary Islands, when the full scale of what had happened aboard the ship was still not yet known.
The National Quarantine Unit at Nebraska Medicine is the only federally funded quarantine facility of its kind in the United States. Its 20 single-occupancy rooms operate under negative air pressure, each with an en suite bathroom, exercise equipment, and WiFi connectivity. The unit was designed for one purpose: housing people exposed to high-consequence pathogens for the full duration of the maximum incubation period, while preventing any possibility of onward transmission. For Andes hantavirus, that maximum window is 42 days, roughly three times longer than the 14-day quarantine periods that became familiar during the COVID-19 pandemic.
Fifteen of the Americans were housed in the NQU. Two were monitored at Emory. The eighteenth was a different case. Dr. Stephen Kornfeld, an oncologist who was aboard the Hondius when the outbreak began, tested positive for Andes hantavirus in early May and was admitted to the Nebraska Biocontainment Unit, a higher-security facility built in 2005 and previously activated to treat American Ebola patients evacuated from West Africa in 2014. The confirmed positive test, announced as the case count aboard the Hondius was still climbing, represented the highest-risk scenario the monitoring program had anticipated. A follow-up test returned inconclusive, and Kornfeld was transferred to the NQU. He completed his 42-day monitoring period and was cleared without developing disease.
The broader outbreak produced a more complicated picture. As of mid-June, a total of 13 cases had been identified across multiple countries: 12 confirmed and one probable, with three deaths and a case fatality ratio of roughly 23 percent. More than 600 contacts were identified across 32 countries and territories, each requiring monitoring coordinated through local public health systems. The CDC and HHS did not specify what proportion of those international contacts have now completed their monitoring periods or been cleared.
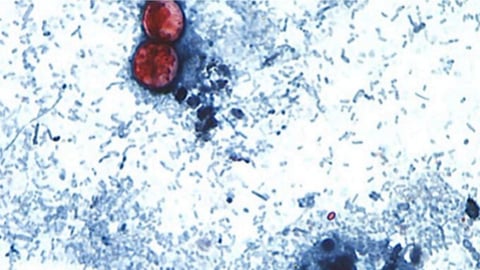
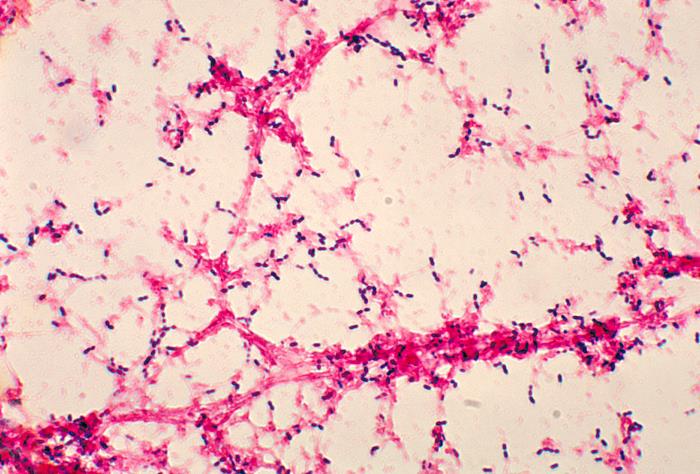
The virus itself is unusual in one medically critical way. Most hantaviruses require direct contact with rodent excreta to infect a person: urine, droppings, or saliva from infected mice or rats. They do not pass between humans. Andes hantavirus, first identified in Chile and Argentina in 1997, is the only known hantavirus strain for which documented human-to-human transmission has been established. That distinction made the containment response aboard the Hondius and in the receiving facilities more complex than a standard rodent-borne outbreak, requiring isolation protocols typically reserved for respiratory pathogens capable of airborne or droplet spread.
The Nebraska Biocontainment Unit and National Quarantine Unit have now been activated three times in eleven years: for American Ebola patients in 2014, for COVID-19 evacuees from Wuhan and the Diamond Princess in 2020, and now for hantavirus patients in 2026. Three distinct pathogens, three distinct clinical protocols, one facility. That no American developed hantavirus disease during the Hondius response, including the one patient who initially tested positive, reflects the accuracy of follow-up testing, the adequacy of the isolation environment, and the monitoring discipline of both the public health staff and the patients themselves. These outcomes are not accidental. They require infrastructure that takes years to build and staff who drill for scenarios they hope never to use.
What the outcome cannot answer is what happened aboard the Hondius before the outbreak was identified. The ship’s South Atlantic route covered remote waters where exact exposure timelines are difficult to reconstruct. How passengers came into contact with a virus primarily associated with rodents in South America’s southern cone remains a question the official record has not fully resolved. Whether crew members were exposed before passengers, and through which mechanism the initial infections occurred, is not publicly established.
The 18 Americans are home. The facilities in Omaha are back on standby. Andes hantavirus remains endemic in the rodent populations of the Southern Cone, and the species that carry it are not in decline. The U.S. response concluded not because the underlying threat was eliminated, but because 42 days passed and no one who came to Nebraska got sick. In outbreak medicine, that is the outcome the infrastructure was built to produce.